
Blog

Subscribe to receive our free Beginner's Guide to Psychedelic Integration.
Happiness Is About Prediction, Not Pleasure
Happiness isn’t about what you get—it’s about what changes.
This paper argues that your brain tracks the difference between expectation and reality, and your emotional state reflects whether things are improving or getting worse.
Feeling good isn’t about having more.
It’s about things getting better.
What “The Predictive Dynamics of Happiness and Well-Being” reveals about the mind
https://journals.sagepub.com/doi/full/10.1177/17540739211063851
Most of us think happiness is simple:
Get what you want → feel good
Lose what you want → feel bad
But according to the paper “The Predictive Dynamics of Happiness and Well-Being”, that picture is incomplete.
Happiness isn’t just about outcomes—it’s about how your brain tracks change over time. (Sage Journals)
And that shift—from outcomes to dynamics—changes everything.
The Core Idea: Your Brain Is a Prediction Machine
The paper is built on a framework called predictive processing.
In this view:
The brain constantly predicts what will happen
It compares predictions to reality
It updates itself based on the difference (called prediction error)
If predictions are accurate:
You stay stable
You achieve your goals
If they’re off:
You adapt
This system isn’t just about perception.
It’s about how you live your life. (Sage Journals)
Happiness = Error Dynamics
Here’s the key insight:
Happiness is not the reward itself—it’s the change in prediction error over time. (Sage Journals)
That means:
If things are getting better than expected → you feel good
If things are getting worse than expected → you feel bad
In other words:
Happiness is about progress, not just outcomes.
This explains why:
A small improvement can feel amazing
A big reward can feel empty if expected
Why Getting What You Want Doesn’t Last
This model explains a familiar problem:
You achieve something you wanted… and the happiness fades.
Why?
Because:
Your brain updates its predictions
The new outcome becomes the baseline
There’s no longer a “positive error”
So the feeling disappears.
Happiness depends on change, not possession.
Mental Health as a Prediction Problem
The paper makes a bold claim:
Mental health depends on how well your brain’s predictive model regulates your actions. (Sage Journals)
In healthy systems:
Predictions are flexible
Errors are updated effectively
Behavior adapts
In unhealthy systems:
Predictions become rigid
Errors are ignored or misinterpreted
Patterns get stuck
This leads to:
Depression → expectations don’t improve
Anxiety → constant negative predictions
Addiction → rigid reward expectations
The Role of Emotion (Valence)
The paper redefines emotion in a precise way.
Instead of:
“Good vs bad feelings”
It proposes:
Emotion (valence) reflects how prediction errors are changing over time. (Sage Journals)
So:
Positive emotion → errors decreasing (things improving)
Negative emotion → errors increasing (things worsening)
Emotion becomes a feedback signal guiding behavior.
Well-Being vs. Momentary Happiness
The paper distinguishes two levels:
1. Momentary Happiness
Short-term fluctuations
Based on immediate prediction changes
2. Long-Term Well-Being
Stability of the overall system
Ability to adapt and maintain progress
Well-being isn’t constant pleasure.
It’s:
A system that can continue improving over time.
The Danger of “Bad Bootstraps”
One of the most interesting ideas is something called bad bootstrapping.
This happens when:
The brain builds a model based on limited or distorted information
Then reinforces it over time
Example:
“I’m not good enough” → shapes behavior → confirms itself
This creates:
Rigid patterns
Self-reinforcing loops
Sound familiar?
This connects directly to modern theories of:
Depression
Anxiety
Cognitive bias
The Sweet Spot: Metastable Flexibility
The paper introduces a powerful concept:
Healthy minds are metastable—stable enough to function, flexible enough to change.
Too rigid:
You get stuck
Too unstable:
You lose coherence
The goal is balance:
Predict well
But stay open to updating
The Bigger Picture
This framework connects deeply with other ideas you’ve explored:
Predictive brain (Andy Clark) → perception as prediction
REBUS / psychedelics → loosening rigid beliefs
Entropic brain → increasing flexibility
This paper adds something crucial:
A model of how happiness itself works inside that system.
Final Take
Happiness is not a reward.
It’s not something you “have.”
It’s something your brain computes—based on how things are changing relative to expectation.
You feel good when things are getting better than expected.
You feel bad when they’re getting worse.
And long-term well-being?
That’s not about constant pleasure.
It’s about maintaining a system that can:
Learn
Adapt
And keep improving
Miller, M. , Kiverstein, J. Rietveld, E., (2022) The predictive dynamics of happiness and well-being, Sage Journals, 14(1) , January 2022, Pages 15-30, https://doi.org/10.1177/17540739211063851
A Recommended Read: The Immortality Key
Brian Muraresku's The Immortality Key argues that ancient Greek mystery rites and possibly early Christian practice involved psychoactive substances — a provocative claim that's strongest on the Eleusinian Mysteries and more contested on early Christianity. A therapist on what the book gets right, what's still debated, and why the deeper question it raises matters for anyone holding contemporary psychedelic experience.
There's a book worth knowing about if you're sitting with questions about the role of direct experience in religious and spiritual life — and about whether the way humans have always related to the sacred has more in common with contemporary psychedelic experience than mainstream religious history tends to admit.
It's called The Immortality Key: The Secret History of the Religion with No Name, by Brian Muraresku. Published in 2020 by St. Martin's Press, with a foreword by Graham Hancock, it argues a provocative thesis: that some of the most important religious traditions in Western history — particularly the ancient Greek mystery rites and possibly early Christian practice — involved the use of psychoactive substances to induce profound mystical experiences.
The book is well-researched, vivid, and worth reading. It's also been the subject of significant scholarly debate, and I want to be honest about that, because how you hold this book matters more than what conclusions you reach from it.
What the Book Actually Argues
Muraresku's central focus is on the Eleusinian Mysteries — a secretive initiation ritual that ran for roughly two thousand years in ancient Greece, until the Christianized Roman Empire shut it down in the fourth century CE.
Participants drank a sacred beverage called kykeon and underwent an experience that, by every surviving account, was profoundly transformative. They emerged describing a loss of fear of death, encounters with the divine, and a sense of having seen something fundamental about existence. The roster of participants includes Plato, Cicero, Sophocles, Plutarch, and a substantial fraction of the most influential thinkers of the ancient world.
What was in the kykeon? The traditional scholarly answer has been: probably nothing chemically active. The experience was attributed to ritual, drama, and psychological suggestion. But a counter-tradition, beginning with Albert Hofmann (the chemist who discovered LSD) and the classicist Carl Ruck in the 1970s, has argued that the kykeon may have contained ergot-derived compounds — psychoactive precursors related to what Hofmann later synthesized as LSD.
Muraresku builds on this earlier work, adding archaeological evidence from sites in Spain and elsewhere where chemical analysis has identified ergot residues in ancient ritual vessels. The case for some psychoactive component to some ancient ritual is, at this point, archaeologically more substantive than it was in the 1970s.
The more controversial second half of the book argues that elements of this tradition may have continued into early Christian practice — that some early Eucharistic rituals may have involved psychoactive sacred drinks, and that the institutional Church gradually suppressed this dimension while preserving its outward forms. This is where the book becomes genuinely contested.
What's Strong and What's Weaker
The strong parts. Muraresku's research into the Eleusinian tradition and the broader Greco-Roman use of altered states is substantive. The archaeological evidence on ergot-containing residues at certain ritual sites is real and worth taking seriously. The broader question — whether direct mystical experience, rather than belief alone, was central to ancient religious life — is a genuine and important one. And the book is exceptionally well-written; it reads like an investigative journey rather than an academic treatise.
The weaker parts. The leap from Eleusinian Mysteries to early Christianity rests on a chain of inferences where each link requires the previous one to be correct. The argument that the original Eucharist was psychoactive doesn't have the same evidentiary support as the Eleusis hypothesis. Classicists and historians of early Christianity have raised serious objections — that Muraresku oversimplifies the "pagan continuity thesis" (the idea that early Christian practice continued earlier mystery traditions), that some of his etymological claims don't hold up, and that he presents speculation with the rhetorical force of established history.
Reviewers in academic venues have been notably more measured than the popular reception. The honest summary, I think, is this: the book is a serious investigation that overstates its strongest claims and contains some claims that probably don't hold up. The Eleusis argument deserves continued investigation. The early Christianity argument is more conjectural than the book sometimes suggests.
Why the Book Still Matters
Even setting aside the contested specifics, the book matters because of the underlying question it raises.
For most of the modern era, the dominant Western framing of religion has been doctrinal — religion as a set of beliefs, organized around texts, sustained through institutional practice. The question of whether religious experience was once more centrally experiential — whether direct, often altered states of consciousness were closer to the heart of religious life than the doctrinal frame suggests — is one that mainstream religious history has only recently begun to take seriously.
This question matters enormously for people now considering or integrating psychedelic experiences.
A great many of my clients, and a great many people I encounter in the broader psychedelic conversation, find themselves wrestling with religious and spiritual questions they hadn't expected. They emerge from experiences that feel undeniably religious in character — encounters with what they can only call sacred, dissolution of the self in ways that the mystics described, a sense of having touched something the rational mind can't quite hold.
For some, these experiences fit reasonably well into existing religious frameworks. For others, particularly those who were raised in or have left specific traditions, the experiences raise uncomfortable questions. If I just had what sounds like a religious experience, what does that mean about religion? About my religion? About what religion has always actually been?
Muraresku's book — whatever you ultimately conclude about its historical claims — opens space for these questions in a useful way. It suggests that the experiential dimension of spiritual life may have been more central, for longer, in more traditions, than the modern doctrinal frame suggests. That the rituals and traditions we've inherited may have been organized around experiences not so different from what contemporary research is now studying.
What I'd Take From the Book
A few things worth holding, whether or not you read it:
The question of what religion actually is doesn't have a settled answer, and the experiential dimension of religious life — particularly through altered states — has been more central across human history than most modern accounts acknowledge.
Whatever you conclude about Muraresku's specific archaeological claims, the broader pattern is real: ceremonial use of psychoactive substances in religious and ritual contexts has been documented across many cultures and historical periods. The contemporary psychedelic conversation isn't reinventing something new; it's reconnecting with something old.
The fact that ancient initiates described their experiences in terms that contemporary clinical trial participants now describe almost identically isn't proof of any specific historical claim. But it does suggest that the experiences themselves have a recognizable structure that doesn't depend on the specific cultural framework around them. Something real is being touched, across times and contexts.
And maybe most importantly: a religious frame and a clinical frame are not the only options for understanding profound experience. The work of contemporary integration — whether you're religious, spiritual, secular, or somewhere in between — is partly the work of finding your own honest way to hold what these experiences are, without forcing them into frameworks that don't quite fit.
Where to Find It
The Immortality Key is widely available — bookstores, libraries, audiobook. The audiobook is particularly well-narrated if you prefer that format. The book is long (about 500 pages), and the second half on early Christianity is where most readers either become enthusiastic or skeptical, so it's worth pacing.
For a more academically careful overview of the same territory, you might also look at Andy Letcher's Shroom: A Cultural History of the Magic Mushroom (which is older but more measured), or scholarly work on the Eleusinian Mysteries by Kevin Clinton at Cornell.
If you find yourself sitting with the questions the book raises — about your own spiritual life, about the experiences you've had or are considering, about how to make sense of what direct mystical experience means for someone living in this century — you're welcome to book a consultation.
Why Transformation Happens in Crisis—and How Psychedelics Fit In
Some experiences don’t just affect you—they change you.
The “pivotal mental state” model suggests that during moments of crisis or under psychedelics, the brain enters a hyper-plastic state where rapid transformation becomes possible.
Whether that leads to growth or breakdown depends on what happens next.
What the “Pivotal Mental States” paper reveals about transformation and psychedelics
https://pubmed.ncbi.nlm.nih.gov/33174492/
Some experiences change you gradually.
Others change you all at once.
A sudden realization.
A crisis.
A moment where “something has to give.”
In the paper associated with PubMed ID 33174492, researchers introduce a powerful concept:
A “pivotal mental state” (PiMS)—a temporary condition where the brain becomes highly flexible, allowing rapid and deep psychological change. (Sage Journals)
This idea reframes how we think about both mental illness and transformation.
The Core Idea: A Window for Change
A pivotal mental state is defined by three key features:
High brain plasticity
Increased associative learning
Capacity for major psychological transformation (Sage Journals)
In simple terms:
The brain enters a state where it can reorganize itself quickly.
This is not a permanent condition.
It’s a temporary window—a moment when change becomes possible.
What Triggers a Pivotal State?
The paper suggests a two-stage process:
1. Chronic Stress (The Primer)
Long-term pressure builds
Emotional and cognitive systems become strained
2. Acute Stress (The Trigger)
A crisis or intense experience occurs
The system destabilizes
This combination creates a tipping point:
A moment where the brain becomes open to radical change. (Sage Journals)
Two Possible Outcomes: Growth or Breakdown
One of the most important insights:
Pivotal mental states are not inherently good or bad.
They can lead to:
Positive Outcomes
Personal growth
New perspectives
Psychological healing
Negative Outcomes
Delusions
Psychosis
Maladaptive beliefs
The difference depends on:
Environment
Support
Interpretation of the experience
Psychedelics: Triggering the Same Mechanism
The paper draws a strong connection between pivotal states and psychedelics.
Specifically:
Psychedelics act on the 5-HT2A serotonin receptor
This increases brain plasticity and sensitivity
It reliably induces a PiMS-like state (Sage Journals)
In other words:
Psychedelics may activate a natural brain mechanism designed for transformation.
They don’t create something new.
They amplify something already built into the system.
Why the Brain Has This System
The authors propose an evolutionary explanation.
When an organism faces:
Extreme stress
Environmental change
Crisis
It may need to rapidly update its behavior or beliefs to survive.
A pivotal mental state allows:
Old patterns to loosen
New ones to form quickly
This makes it a high-risk, high-reward adaptation.
Mental Illness Through This Lens
This model offers a new way to understand conditions like:
Depression
Anxiety
Psychosis
Instead of viewing them only as dysfunctions, the paper suggests:
They may involve dysregulated pivotal states.
For example:
A PiMS triggered without support → negative outcomes
A PiMS guided properly → positive transformation
Why Context Matters So Much
Because pivotal states are so sensitive, context becomes critical.
The same state can lead to:
Healing in a safe, structured environment
Harm in a chaotic or unsupported one
This directly supports a core principle in psychedelic therapy:
Set and setting determine outcomes.
A New Model of Transformation
The paper shifts focus from outcomes to process.
Instead of asking:
Why do people change?
It asks:
What state enables change to happen?
And the answer is:
A temporary, hyper-plastic state where the brain becomes open to reorganization.
The Bigger Picture
This idea connects with several major theories:
REBUS → relaxing rigid beliefs
Entropic brain → increasing flexibility
Neuroplasticity → enabling change
But it adds something new:
A model for when and why transformation happens at all.
Final Take
The concept of pivotal mental states reframes both crisis and healing.
It suggests that:
Moments of instability are also moments of possibility
The brain has built-in mechanisms for radical change
Psychedelics may tap directly into those mechanisms
And perhaps most importantly:
Transformation doesn’t happen gradually—it happens when the system becomes flexible enough to allow it.
Brouwer A, Carhart-Harris RL. Pivotal mental states. J Psychopharmacol. 2021 Apr;35(4):319-352. doi: 10.1177/0269881120959637. Epub 2020 Nov 11. PMID: 33174492; PMCID: PMC8054165.
A Recommended Read: How to Change Your Mind
Michael Pollan's How to Change Your Mind is the most accessible mainstream introduction to contemporary psychedelic therapy and remains worth reading, with some important caveats about what's changed in the field since 2018. A therapist's recommendation and a note on how to read it well.
If you're new to the contemporary conversation about psychedelic therapy and you want one accessible book to start with, this is the one I'd point you toward.
Michael Pollan's How to Change Your Mind: What the New Science of Psychedelics Teaches Us About Consciousness, Dying, Addiction, Depression, and Transcendence, published by Penguin Press in 2018, did more than any other single book to move the contemporary psychedelic conversation from fringe to mainstream. It was a bestseller, became a Netflix documentary series, and has likely been read by more people interested in this field than any other contemporary book on the subject.
It's also a model of careful, curious, journalistically rigorous engagement with material that's easy to either overhype or dismiss. Pollan, a respected writer best known for his work on food and agriculture, came to this topic as a skeptic and a journalist. He researched. He interviewed researchers and patients. He underwent guided experiences himself with LSD, psilocybin, ayahuasca, and 5-MeO-DMT. And he wrote about all of it with the measured, slightly bemused intelligence that's his hallmark.
The book is genuinely worth reading. I want to offer a few observations about how to read it well.
What the Book Does Well
The book traces the history of psychedelic research carefully — the early promise in the 1950s and 60s, the cultural and political backlash, the long suppression, and the cautious renaissance that began in the late 1990s. Pollan is good on the institutional history. He's particularly good on the figures who kept the research alive during the dormant years and the new generation of clinicians who picked it up.
He's strong on the current clinical research, particularly the work at Johns Hopkins, NYU, and Imperial College London on psilocybin for depression, anxiety, end-of-life distress, and addiction. He presents the studies fairly, neither overselling the results nor dismissing them.
He's especially valuable on the experiential dimension. Most journalists who write about psychedelic therapy don't actually undergo the experiences they're describing. Pollan does, and his accounts of his own sessions are some of the most honest and unsentimental writing on the subject. He neither claims to have been transformed in some grand way nor dismisses what happened. He sits with the experiences and lets them be complicated.
And his prose is excellent. The book reads easily, moves at a thoughtful pace, and gives you genuine information without being either dry or breathless. For most readers, it's an ideal entry point.
What to Hold Lightly
A few things to keep in mind as you read.
The book is now seven years old. Published in 2018, it represents a particular moment in the psychedelic conversation — one of cautious optimism, with FDA approval of MDMA-assisted therapy for PTSD seeming imminent and the broader field on a steady upward trajectory. A great deal has happened since. The FDA rejected MDMA-assisted therapy in August 2024 over serious concerns about study design, blinding, and ethical violations. Compass Pathways' psilocybin trials have produced positive Phase 3 results but the regulatory path remains uncertain. The MAPS organization at the center of Pollan's optimistic account has gone through significant institutional changes and ethical reckonings. The book doesn't capture any of this.
The treatment is more optimistic than the current evidence supports. Pollan was writing during a wave of genuine enthusiasm, and the book reflects that. The studies he highlights were promising, but many of the most exciting early findings have proven harder to replicate at scale than the book implies. The field has been forced into a more sobered position since — recognizing that the medicines are real but their integration into clinical care is harder than was hoped.
The mystical experience framing is more contested than the book suggests. Pollan presents the research on mystical-type experiences as central to therapeutic outcomes, and this remains a major theme in the field. But the framing has been challenged — partly by philosophers like Chris Letheby, who argue that the therapeutic value doesn't actually depend on mystical content, and partly by researchers who worry about the ethical implications of treating mystical experience as the active ingredient. Read Pollan's enthusiasm for the mystical-experience framework with some critical distance.
The book doesn't address what the field has since had to learn about ethics and care. The MAPS-related sexual misconduct cases, the journal retractions, the gap between research conditions and real-world clinical implementation — these are real and ongoing concerns that have shaped how careful practitioners now think about this work. The book predates most of this conversation.
Why I Still Recommend It
With those caveats, the book remains the best mainstream introduction to the field, and one of the few that combines historical context, contemporary science, and honest first-person reporting in a single accessible package. Most readers who finish it have a substantially clearer picture of what psychedelic therapy is, why it's being studied, and what's at stake than they did before.
For people considering psychedelic-assisted therapy now, the book is a useful starting point but not a complete guide. You'll want to supplement it with more current sources for the regulatory landscape, the ethical conversations, and the specific clinical considerations that have come into clearer view since 2018.
For people not considering psychedelic therapy but curious about the broader cultural conversation, the book is excellent. It will give you the vocabulary, the history, and the basic clinical picture to follow what's happening as the field continues to develop.
For practitioners new to this space, it's still one of the recommended starting points — though I'd pair it with more recent and more critical literature.
Where to Find It
How to Change Your Mind is widely available — bookstores, libraries, audiobook. The Netflix documentary series based on the book covers similar territory in four hour-long episodes and is also worth watching if you prefer video.
If you find yourself drawn into the larger questions the book raises — about your own potential interest in this work, about how to think clearly about psychedelic experience, about what careful contemporary care actually involves — you're welcome to book a consultation.
The Ego Lives in the Brain
The ego isn’t just an idea.
It may be a brain network.
In this paper, researchers argue that the default mode network underlies our sense of self—and that psychedelics temporarily disrupt it, loosening the rigid patterns that shape how we think, feel, and perceive reality.
What “The Default Mode, Ego-Functions and Free-Energy” reveals about consciousness
https://pmc.ncbi.nlm.nih.gov/articles/PMC2850580/
For over a century, psychologists have debated the nature of the ego.
Is it real?
Is it just a concept?
Or does it have a physical basis in the brain?
In this influential paper by Robin Carhart-Harris, a bold claim is made:
The Freudian idea of the ego may map directly onto a real brain system—the default mode network (DMN).
And that idea has major implications—not just for psychology, but for psychedelics and mental health.
The Core Idea: The Ego Has a Neural Home
Freud described the ego as:
The organizing center of the mind
Responsible for self-control, identity, and reality-testing
Carhart-Harris suggests this isn’t just metaphor.
It may correspond to a specific brain network:
The default mode network (DMN)—active when you’re thinking about yourself, your past, your future, and your identity.
This network includes areas like:
Medial prefrontal cortex
Posterior cingulate cortex
In simple terms:
The DMN may be the biological basis of the “self.”
The Brain as a Prediction Machine
The paper also builds on a broader theory:
The brain works by minimizing uncertainty—what’s called free energy.
This means:
The brain constantly predicts the world
It updates those predictions when they’re wrong
It tries to keep things stable and predictable
The ego (or DMN) plays a key role here:
It maintains a coherent model of “you” in the world
It filters and organizes experience
This keeps reality stable—but also limits flexibility.
When the Ego Becomes Too Strong
A stable sense of self is useful.
But it can also become overly rigid.
The paper suggests that excessive DMN activity may be linked to:
Depression (repetitive negative thinking)
Anxiety (overactive self-monitoring)
Addiction (fixed behavioral patterns)
In these cases:
The brain becomes “stuck” in its own model of reality.
Psychedelics: Quieting the Ego
Here’s where things get interesting.
Research shows that psychedelics reduce activity in the DMN.
The result:
The sense of self weakens
Boundaries dissolve
New patterns of thinking emerge
This is often described as ego dissolution.
From this model, it’s not mysterious—it’s neurological:
Psychedelics temporarily disrupt the brain system that maintains the self.
A Hierarchy of Mind
The paper also proposes a layered view of the brain:
High-level systems (like the DMN) → abstract thinking, identity
Lower-level systems → emotion, sensation, basic drives
Normally:
High-level systems dominate
Under psychedelics:
Lower-level signals gain influence
This creates:
More emotional intensity
More sensory richness
Less rigid interpretation
Primary vs. Secondary Consciousness
The paper introduces a key distinction:
Secondary consciousness
Normal waking state
Structured, controlled, ego-driven
Primary consciousness
Dreaming, early development, psychedelic states
More fluid, less constrained
Psychedelics shift the brain toward primary consciousness.
That’s why experiences feel:
More imaginative
Less logical
More emotionally raw
Bridging Freud and Neuroscience
One of the most compelling aspects of the paper is its attempt to connect:
Psychoanalysis (Freud)
Modern neuroscience
Freud described:
The ego
The unconscious
Internal conflict
This paper suggests:
These may correspond to real brain systems and dynamics.
It’s not that Freud was entirely right—but that his ideas may have been early descriptions of real biological processes.
Why This Matters
This framework helps explain:
1. Psychedelic Therapy
Disrupting the ego may allow new perspectives
Patients can break out of rigid thought patterns
2. Mental Illness
Disorders may involve overly rigid self-models
Treatment may require loosening, not just correcting
3. Consciousness Itself
The self is not fixed
It’s a process generated by the brain
Final Take
This paper marks a turning point.
It suggests that:
The ego is not just a psychological concept
It’s a neural system
And it can be altered
Psychedelics don’t just change what you see.
They change who is doing the seeing.
And in that shift, something important becomes clear:
The self you experience every day is not a fixed thing—
it’s something your brain is actively maintaining.
Carhart-Harris RL, Friston KJ. The default-mode, ego-functions and free-energy: a neurobiological account of Freudian ideas. Brain. 2010 Apr;133(Pt 4):1265-83. doi: 10.1093/brain/awq010. Epub 2010 Feb 28. PMID: 20194141; PMCID: PMC2850580.
Consciousness Begins with Feeling
Neuropsychoanalyst Mark Solms argues that consciousness doesn't begin with thinking — it begins with feeling, generated by ancient brainstem structures that monitor the body and produce the affective signals that motivate all behavior. A therapist on what this framework means for healing, why thinking alone often fails to reach what hurts, and why depth-oriented and psychedelic work aim at the feeling layer rather than the thinking one.
There's a quiet conviction that runs through most modern theories of consciousness, and it goes something like this: consciousness is something the cortex does. The folded, gray, evolutionarily recent outer layer of the brain. That's where perception happens, where thought happens, where the self gets constructed. The rest of the brain — the brainstem, the older structures we share with much simpler animals — serves consciousness without being where consciousness lives.
In The Hidden Spring: A Journey to the Source of Consciousness, the neuropsychoanalyst Mark Solms argues that this conviction has the picture exactly inverted.
Consciousness, he proposes, doesn't begin with the cortex. It begins with the brainstem. Not with thinking. With feeling. The raw affective states that animals experience long before they develop anything like cognition — pleasure, pain, hunger, fear, the felt urgency of being alive — are not the byproducts of consciousness. They are its source.
This is not a minor adjustment. It's a fundamental reframing of where awareness actually lives, what it's for, and what kind of work we should expect to do if we want to change it. I want to walk through Solms's argument because I think it gives a neurological home to something good clinicians have always known: that real psychological change has to reach the feeling layer, not just the thinking one. And it changes how we should understand what depth-oriented and psychedelic work are actually doing.
What Solms Is Actually Claiming
Mark Solms is an unusual figure. He's both a neuropsychologist with serious credentials and a trained psychoanalyst. He founded the field of neuropsychoanalysis, which has spent decades trying to bring Freud's clinical insights into productive conversation with contemporary brain science. His new book is, in some sense, the culmination of that project.
His central claim is built on a body of clinical evidence that the cortical-consciousness mainstream has long had trouble explaining.
Patients with severe cortical damage — including, in some cases, near-total loss of cortical function — can remain awake, responsive, emotionally expressive, and recognizably aware in ways that the cortical theory predicts they should not be. Children born without significant cortex (hydranencephaly, for instance) show clear signs of pleasure, distress, recognition, and affective life. They smile at their mothers. They cry when in pain. They orient to comforting voices. By the standards of the cortical theory, they shouldn't be conscious at all. By the standards of anyone who has actually met them, they clearly are.
Damage to specific brainstem structures, on the other hand, can eliminate consciousness entirely — even when the cortex is fully intact. The brainstem isn't just supporting consciousness from below. Damage there abolishes awareness in ways that no amount of cortical damage seems to fully achieve.
What does this evidence point to? Solms argues that consciousness is generated, fundamentally, by a small set of brainstem structures whose job is to monitor the body's internal state and produce the felt signals that motivate behavior. The cortex isn't where consciousness lives. The cortex is what consciousness uses — to elaborate, to think, to plan, to remember. But the consciousness itself — the basic felt sense of being alive, of mattering to oneself, of caring about what happens — comes from somewhere deeper.
And what comes from that deeper place isn't thought. It's feeling.
Why Feeling Comes First
The evolutionary logic here is compelling once you sit with it.
Animals had affective states — pleasure, pain, hunger, satisfaction — long before they had anything resembling cognition. The very simplest organisms have to be able to move toward what helps them and away from what harms them. To do that, they need some kind of internal signal that distinguishes good from bad — some felt valence that motivates behavior. Without it, no organism survives. The capacity to feel something as good or bad is, in this view, the most ancient and fundamental form of consciousness.
Thinking, by contrast, came much later. Higher cognition — abstract reasoning, language, self-reflection — is a recent evolutionary development, dependent on cortical structures that most animals don't have. If consciousness required cognition, most of the living world wouldn't be conscious. Solms argues, with the affective-neuroscience tradition that goes back to Jaak Panksepp, that this conclusion gets the picture backward. Most animals are conscious. They just feel without thinking the way we do.
What we add, with our developed cortex, isn't consciousness. It's the elaboration of consciousness into thought, narrative, planning, self-reflection. The cortex is what allows us to think about our feelings. But the feelings themselves — and the consciousness that goes with them — predate the cortex and don't depend on it.
This is why, in this view, consciousness is fundamentally about valuing the world rather than representing it. The basic question consciousness exists to answer isn't what's out there? It's what should I do? What helps me? What harms me? Feeling is the answer. Thought is a later, much more elaborate way of refining the same basic project.
The Implication for the Self
If Solms is right, then the self isn't primarily a thinking thing. It's primarily a feeling thing.
The "core self," in this view, is built from affective signals about the body's state. Whether you're hungry, tired, safe, threatened, satisfied, longing, grieving, content. These bodily and emotional states are what produce the foundational sense of being you — alive, mattering to yourself, with a stake in what happens next.
The thinking self — the narrative self, the verbal self, the self that has opinions and remembers stories and plans the future — is layered on top of this affective core. It depends on the core for its substance. Without the underlying affective life, the thinking would have nothing to be about. The cortex elaborates what the brainstem cares about. Without the caring, the elaborating has no meaning.
This is, in some sense, a return to something Freud knew but couldn't yet ground neurologically — that the unconscious is older and more fundamental than the conscious, that what drives behavior is rarely what we can articulate, and that the talking mind we identify with is a relatively thin layer sitting on top of much deeper systems. Solms is one of the few contemporary neuroscientists making the explicit bridge between modern brain science and this older psychoanalytic understanding.
What This Means Clinically
For clinical work, the implications are significant.
Most contemporary psychotherapy operates primarily at the cortical layer — working with thoughts, beliefs, narratives, cognitive patterns. Cognitive behavioral therapy treats the thoughts. Many forms of psychoanalytic and psychodynamic therapy work with the narrative self. Even much depth therapy operates more verbally than it sometimes acknowledges.
If Solms is right, this often misses where the issue actually lives.
The depression that won't lift through better thinking. The anxiety that persists despite clear cognitive understanding. The trauma that survives every insight. These aren't failures of the thinking mind to grasp something. They're conditions of the affective core — patterns in the deeper system that the cortex can't directly access or modify.
This is why so many of my clients come in having done years of good therapy and still feel that the work hasn't quite reached the layer where the actual suffering is. They understand their patterns. They can name their triggers. They know what their parents did and didn't do. And the feelings haven't changed. The body still braces. The chest still tightens when certain emails arrive. The sleeplessness continues. The thinking layer has been worked on, sometimes extensively. The feeling layer — where Solms locates consciousness itself — hasn't been touched.
This is part of why somatic approaches, depth-oriented therapy with attention to affect, body-based work, and contemplative practice reach things that cognitive therapy alone can't. They work with the affective core directly — not by talking about feelings but by attending to them, allowing them, sometimes provoking and metabolizing them.
It's also why the therapeutic relationship itself matters so much. Two people in attuned interaction regulate each other at the level of the affective core, not just the thinking mind. The presence of a steady, attuned, regulated other does work that no amount of insight alone can replicate.
What This Means for Psychedelic Work
Solms's framework also illuminates something specific about psychedelic-assisted therapy that the predictive-processing accounts only partially capture.
Psychedelics, of course, do loosen predictive models — that's been one of the most important neuroscientific findings of the last fifteen years. But what people actually report, during and after these experiences, isn't primarily that their predictive models changed. It's that they felt something — sometimes for the first time in years. Grief that had been frozen begins to flow. Love that had been intellectually known becomes directly felt. Fear that had been managed becomes accessible. The whole affective layer that the thinking mind has been managing from a distance comes into immediate contact.
In Solms's framework, this makes sense. The medicines don't just affect cognition. They open access to the deeper affective systems where consciousness actually lives. The therapeutic value isn't only about reorganizing beliefs. It's about restoring access to the feeling layer that's been suppressed, walled off, or numbed for years.
This is why integration of psychedelic experiences has to attend to the affective dimension specifically. The thoughts that arose during the experience can fade. The narrative interpretations can dissolve. But the felt experience of having met grief, having felt love, having been moved at the level where one is moved — these can produce lasting change if they're supported, allowed to land, integrated into ongoing emotional life. Not as memory of an experience. As permission to feel again in ordinary time.
Where the Framework Is Still Contested
I want to be honest: Solms's argument is provocative and not universally accepted.
The mainstream of consciousness research continues to focus primarily on cortical processes. Many researchers find Solms's brainstem-centered model too speculative or too dependent on contested interpretations of the clinical evidence. The debates between cortical and subcortical theories of consciousness are real and unresolved.
Solms is also engaged in an ambitious project that goes beyond pure theory — he's been working with collaborators to build a computer model of consciousness based on his framework, in part to test whether his theoretical claims can produce something that behaves recognizably the way conscious systems do. This is interesting and ongoing work, and its results will eventually matter for evaluating his framework. For now, the model is in development and the theoretical claim remains debated.
What I find valuable about Solms, regardless of where the scientific debates eventually land, is the clinical orientation he brings. As both a neuroscientist and a psychoanalyst, he's spent decades sitting with patients whose suffering doesn't reduce to cognitive errors. He's taken seriously the clinical evidence that we are feeling beings before we are thinking ones, and that the work of healing usually has to reach the feeling layer to produce change that lasts. The neurological framework gives a home to insights that clinicians have always known. Whether the framework turns out to be right in its specifics, the clinical orientation seems to me correct.
A Closing Thought
The deepest implication of Solms's work, I think, is this: you are not primarily a thinking thing. You are a feeling organism that thinks.
This isn't a diminishment. It's a more accurate placement. The thinking is real and important and uniquely human. But it's built on top of something older, deeper, more fundamental. The capacity to care about what happens. The felt sense of being alive. The motivational urgency that drives every choice you make.
Healing, in this view, isn't primarily about thinking better. It's about restoring contact with the feeling layer that has been managed, suppressed, or walled off — and learning, slowly, to live from that layer rather than from the cortical management that has been keeping it at bay.
Good therapy at depth attends to this. So does contemplative practice, when it's serious. So does the kind of careful work that psychedelic-assisted therapy aims toward. None of these are primarily projects of changing your mind. They are projects of returning you to your feeling.
If you'd like a place to do that work, you're welcome to book a consultation.
The Mind Is Not a Window: What Huxley Got Right About Psychedelics
In 1954, Aldous Huxley proposed that the mind is a filter, not a window — and that psychedelics temporarily loosen that filter, with consequences that can be heavenly or hellish. A therapist on what Huxley got right, what modern neuroscience has refined, and where the field actually is right now in the messy work of bringing these substances into mainstream medicine.
In 1954, long before brain scans or clinical trials, Aldous Huxley took mescaline and wrote something that still feels slightly dangerous to read.
He suggested that your mind is not a window onto reality. It's a filter.
In his book The Doors of Perception, Huxley proposed that the brain functions as a "reducing valve" — screening out most of what's actually there so you can survive, function, and not be overwhelmed. Psychedelics, he argued, temporarily loosen that filter, letting through what's normally screened out.
Two years later, in Heaven and Hell, he expanded the idea. When the filter opens, what comes through isn't always beautiful. Sometimes it's radiant, transcendent, luminous. Sometimes it's terrifying. He called it heaven and hell. Today we might call it altered states of consciousness — and we'd note, more clinically, that the same opening can produce both.
What's striking, seventy years later, isn't that Huxley wrote any of this. It's how close modern neuroscience has come to taking him seriously — and where it has departed from him in important ways. I want to walk through both, because Huxley's framework still illuminates something the more technical accounts don't quite reach, and because the current moment in psychedelic medicine asks us to hold both his insights and their limits.
The Filter, Translated
Huxley didn't have the vocabulary of receptors or neural networks. He was writing as a literary man with a deep curiosity about what his own mind was doing. But if you translate his idea into contemporary terms, it lands in a familiar place.
Modern psychedelic research — particularly work on psilocybin — suggests that these compounds disrupt the brain's normal patterns of organization. Activity becomes less synchronized. Networks that ordinarily operate in tight coordination begin to loosen. The brain, in a real sense, becomes less constrained by its own habitual structures.
Researchers wouldn't say the brain is revealing ultimate reality. That's a metaphysical claim, and science is careful about those. But they would say something adjacent: psychedelics appear to reduce rigid patterns of perception, thought, and self-representation. The familiar filters loosen.
That's not exactly a reducing valve in Huxley's sense. He thought the filter was protecting us from too much truth. Modern neuroscience tends to say the brain maintains efficient models of the world, and psychedelics temporarily destabilize those models. Same shape, different language.
The difference matters philosophically — but for the lived experience of someone taking these compounds, it makes little difference. Whether you call it filter dissolution or model destabilization, the result is the same: the world looks different. Things that were ignored become vivid. Things that were certain become uncertain. The construction becomes briefly visible as a construction.
When a Chair Stops Being a Chair
One of the strangest passages in The Doors of Perception is also the simplest.
Huxley looks at a chair. Not metaphorically, not symbolically — just a chair. And he becomes transfixed, not by what it means or what it's for, but by what it is. Its color. Its form. Its sheer presence. He calls this is-ness — a direct encounter with existence, stripped of utility and interpretation.
This sounds mystical. But you can map parts of it onto modern cognitive science.
Under psychedelics, salience shifts. The brain stops prioritizing what's useful and starts amplifying what's there. Categories loosen. Familiar things become strange, vivid, emotionally charged. The chair stops being a chair-for-sitting and becomes simply this remarkable, present object that you've been walking past for years without seeing.
For some people, this shift is transformative. They describe seeing their own children, their partners, the trees outside their window, the food on their plate — as if for the first time. The veil of habituation thins, and the world comes back through with its color saturated.
This is one of the things that gives psychedelic experiences their reputation for being revelatory. Not because the world changed, but because the layer of automatic processing that filters how you experience it briefly thinned. What's already there can be encountered more directly.
Heaven and Hell Weren't Metaphors
In Heaven and Hell, Huxley insists that visionary states are not inherently positive. The same mechanisms that generate beauty can generate horror.
Modern research agrees, in a more clinical tone.
Psychedelics can produce deep emotional insight, a sense of unity or meaning, and what some describe as the most important experiences of their lives. They can also produce anxiety, terror, confusion, and lasting destabilization. The same compound, in the same person, can be radiant one week and horrific the next, depending on what's going on inside and around them.
This is why contemporary research emphasizes set and setting — the psychological mindset and physical environment in which the experience occurs. It's not a soft variable. It's central to outcomes. Huxley intuited this decades before clinical research could quantify it.
What he understood is that these states are not just pharmacological events. They are total experiences, shaped by context, expectation, interpretation, and the inner world of the person having them. The same opening can lead to liberation or destabilization depending on what surrounds it.
This matters clinically. The careful work of preparing someone for a psychedelic experience, providing a safe and supportive environment, and integrating what arises afterward isn't ornamental. It's the difference between a heavenly experience and one that adds to suffering.
Where the Science Got Practical
The real shift from Huxley's era to now is not philosophical — it's clinical. The questions changed.
Researchers stopped just asking what is consciousness? and started asking: can changing consciousness treat disease?
The most compelling evidence so far is in depression. Psilocybin-assisted therapy has shown the ability to produce rapid reductions in depressive symptoms in some patients, particularly when paired with structured psychological support. There's also growing research into addiction — including alcohol use disorder, smoking cessation, and other substance use patterns — and into anxiety, end-of-life distress, and treatment-resistant conditions where standard approaches have not produced full relief.
The early results have been striking enough to drive significant investment, both scientific and commercial. Major academic centers have established psychedelic research programs. Pharmaceutical companies have invested heavily. Phase 3 trials are underway for multiple compounds. Some U.S. states — most notably Oregon and Colorado — have moved forward with legal psilocybin therapy programs ahead of federal action.
But the field is far from settled. And recent events make this clearer than they have in years.
What the FDA Decision Revealed
In August 2024, the FDA rejected MDMA-assisted therapy for PTSD — the first time a Schedule I psychedelic had come before the agency for medical approval. The decision surprised many in the field, who had assumed the strong clinical results and significant need would carry the application through.
The concerns the FDA raised were substantial. Study design problems. Issues with blinding — meaning patients and therapists could often guess who had received the drug versus a placebo, which compromises the science. Allegations of sexual misconduct during one of the midstage trials. Lack of standardization in the psychotherapy component, which the FDA noted would make the treatment difficult to reproduce reliably if approved.
Some of these were issues with one specific company's specific application. But some were deeper concerns about the field itself — about how to study treatments where the subjective experience is part of the therapy, how to ensure rigorous trials when participants can usually tell whether they got the drug, and how to standardize a treatment that involves both pharmacology and skilled psychological support.
The rejection sent shockwaves through psychedelic medicine. It signaled that the path to FDA approval would be longer, more expensive, and more uncertain than many had hoped.
As of mid-2026, the next major test is Compass Pathways' psilocybin therapy for treatment-resistant depression. After two positive Phase 3 trials, the company is moving toward a New Drug Application that could result in psilocybin becoming the first FDA-approved classical psychedelic — potentially by late 2026 or early 2027. But the path is not guaranteed. The FDA has made clear it will not lower its standards. The political and regulatory landscape continues to shift.
This is the current state: high potential, incomplete validation, and a field reckoning with the gap between what individual experiences suggest and what rigorous clinical evidence requires.
What Huxley Saw, and What He Couldn't See
Huxley didn't prove that psychedelics reveal a deeper layer of reality. That question is still open, probably unanswerable in scientific terms.
But he did get several things right that the more careful, technical accounts can sometimes miss:
That perception is not neutral; it is filtered.
That changing consciousness changes meaning, not just sensation.
That altered states are structured, not random — they follow particular patterns.
That the same mechanism can produce beauty or terror, depending on what surrounds it.
That what we call reality is, in significant part, negotiated by the brain.
What Huxley couldn't see, of course, is everything that's happened in the seven decades since. He didn't see the careful clinical trials that have begun to specify what psychedelics actually do. He didn't see the failures — the recreational use that has harmed many people, the unregulated retreats where things have gone badly, the regulatory rejections of work that wasn't quite ready. He didn't see the careful contemporary practitioners who have learned that the experience is only one part of a longer process, and that integration is often where the real change happens.
If Huxley were writing today, I suspect he would refine his framework rather than abandon it. The filter loosens, yes. What comes through can be heaven or hell, yes. But what happens to the experience afterward — how it's held, witnessed, supported, integrated into a life — turns out to matter at least as much as the experience itself.
What This Means for the Current Moment
For people considering psychedelic experience now, in this in-between time before legal frameworks are fully in place, a few things seem worth holding:
The experiences are real. They can be genuinely transformative. The clinical evidence supports their potential, particularly for conditions that haven't responded to other treatments.
They are also not guaranteed. Heaven and hell are both possibilities. The same compound, the same setting, the same intention can produce profoundly different experiences in different people, or in the same person at different times.
What surrounds the experience matters as much as the experience. Set, setting, preparation, support, integration. Without these, even powerful experiences often fade or destabilize. With them, ordinary experiences can become foundational to lasting change.
The field is still figuring itself out. The MDMA rejection has been a reset. The questions about study design, standardization, and the role of the therapeutic component are real. Anyone telling you they have it all figured out — whether they're selling a retreat, a treatment, or a worldview — is probably overstating the case.
Patience is part of the work. The dream of a quick fix through pharmacology is older than psychedelic medicine. It has never been quite right. What these compounds offer is a particular kind of opening, the value of which depends on what's done with it, by whom, over what kind of time.
A Closing Thought
What I find most enduring about Huxley's work — even where it overreaches, even where science has moved past it — is its acknowledgment of how much we don't know about consciousness, including our own.
The mind we live with is more constructed than it feels. The world we perceive is more filtered than we realize. The self we identify with is more elaborate and more recent than we tend to believe. These observations are humbling, and they should be.
But they're also liberating. If experience is filtered, the filter can sometimes thin. If perception is constructed, the construction can sometimes shift. If the self is a model, the model can sometimes update.
This is what Huxley glimpsed in his armchair in 1954, and what modern neuroscience is still working to understand. Not that psychedelics open a door to another world — but that they reveal how constructed this one already is, and how much room there might be for it to be experienced differently.
That insight doesn't require taking anything. It's available, in quieter forms, to anyone willing to attend carefully to their own mind. The compounds may speed the recognition. The recognition itself is older than any of them.
If you're sitting with the questions Huxley raised — about your own perception, your own self, the patterns that have organized your experience — and you'd like a place to explore them carefully, you're welcome to book a consultation. The work is real. It moves at the pace it moves. And it does not require certainty about questions that may not have certain answers.
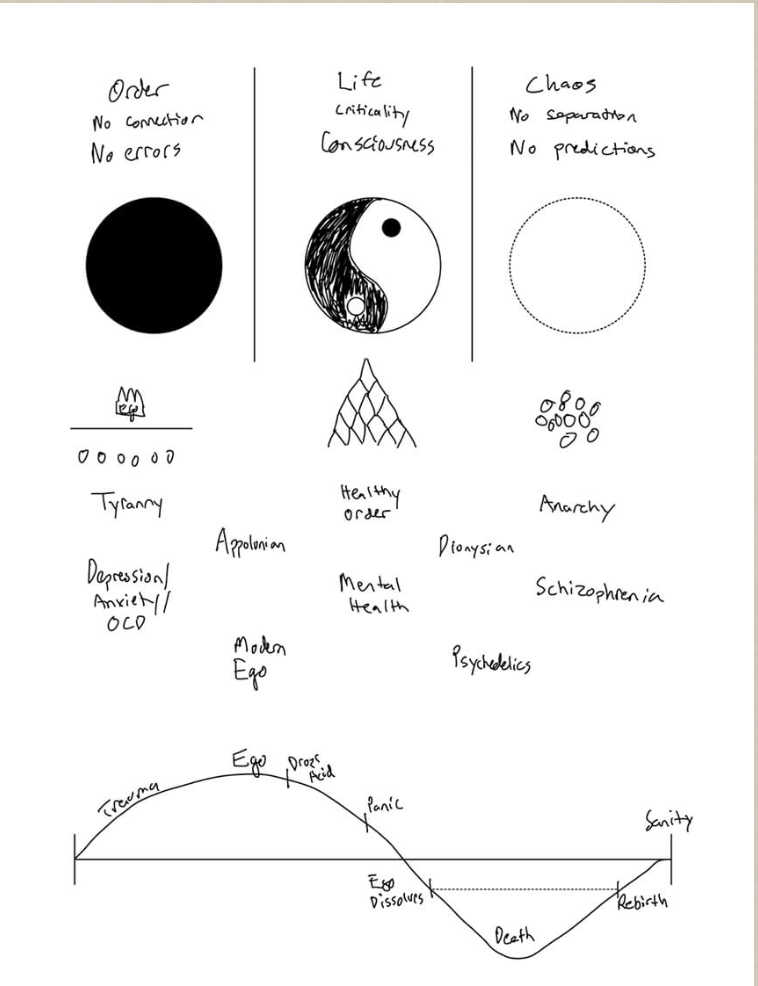
Order, Chaos, and the Story of Becoming
The same shape recurs across mythology, contemplative practice, psychotherapy, storytelling, and now neuroscience: transformation requires passing through a period of descent before a new configuration can emerge. A therapist on the universal arc of becoming, and why what feels like falling apart is often the necessary phase of real change.
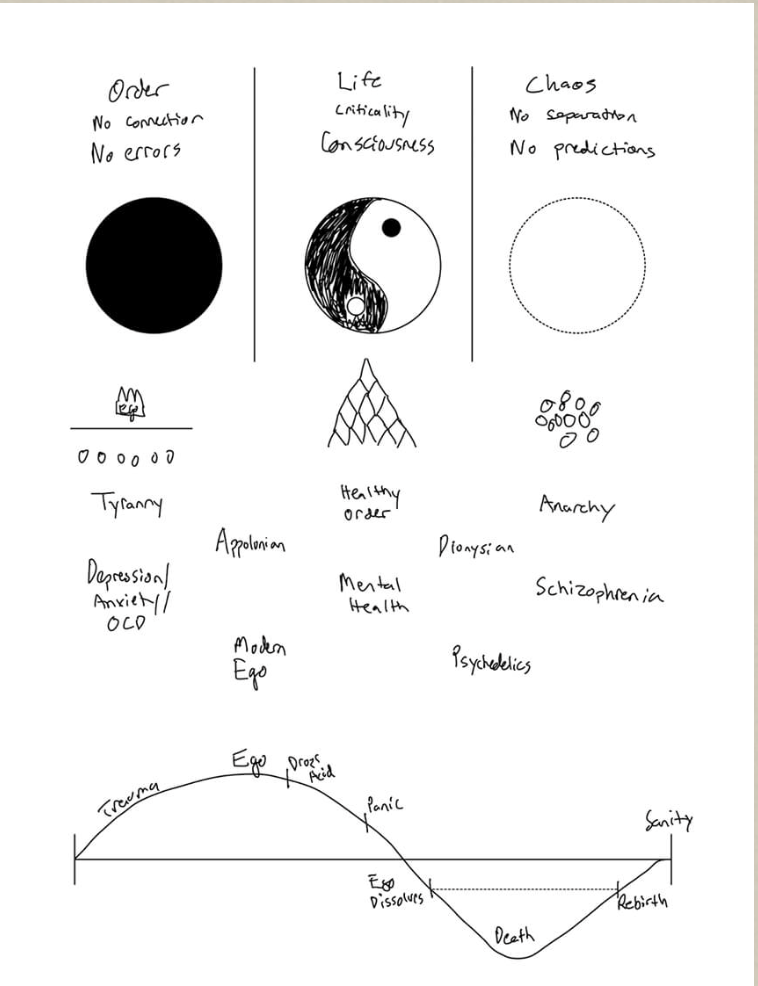
Illustrations from Guy Trefler, showing the applications of the spectrum across life, mind, and society.
There's a particular shape that transformation takes.
It's the shape Joseph Campbell traced through the world's myths and called the hero's journey. The shape Carl Jung mapped through the alchemists, calling it individuation. The shape trauma therapists watch their clients move through, sometimes over years. The shape every meaningful film follows, whether the screenwriter knows it or not. The shape contemplative traditions across cultures have described for thousands of years.
It's also the shape modern neuroscience is now describing, in the language of entropy, neural flexibility, and reorganization.
I want to walk through this shape, because once you see it, a lot of what looks like falling apart turns out to be something else. And once you can recognize when you're inside it, the experience changes — not because it becomes easier, but because you can stop interpreting it as failure.
What the Shape Actually Is
The shape isn't a straight line. It's a curve, and it has five recognizable phases.
Stability. A system — a person, a relationship, a culture, a way of being — has organized itself into a coherent form. There's an identity. A worldview. A set of patterns that work, more or less. The system can predict itself and its world.
This phase has gifts. Continuity. Function. The ability to plan. Most of life is lived inside it, and most of the time, it's where life should be lived. You can't grow continuously. You need long stretches of stability for the previous transformation to consolidate.
Disruption. Something breaks. A loss. A crisis. A relationship ending. A diagnosis. A profound experience — including, for some people, a psychedelic one. An illness. A truth that can't be unseen. A child leaving home. The death of a parent. The slow accumulating recognition that the life you've been living isn't quite yours.
The stable system meets something it can't absorb without changing.
Descent. This is the hardest phase, and the one most people don't realize is a phase. The structure that had been holding you starts to fail. The patterns don't quite work. The identity that had been clear becomes uncertain. You can't yet see what's coming, and you can't quite stay where you were.
In psychological terms, this is when the old self starts to dissolve before the new self has formed. It often feels like falling apart, like depression, like losing your mind. People in this phase frequently believe something is terribly wrong with them — that they've broken, that they need to be fixed, that they should be working harder to hold it together.
The mythological traditions call this the underworld. The contemplative traditions call it the dark night of the soul. Jung called it the descent. The neuroscience would call it the entropic phase — the period when the old configuration has loosened and the new one hasn't yet stabilized.
It is genuinely difficult. It is also genuinely necessary. There is no way to the new configuration except through this.
Letting Go. Somewhere in the descent, a shift happens. The person stops fighting what's been dissolving. They stop trying to put the old structure back together. They allow themselves to not know what comes next.
This isn't giving up. It's something closer to surrender — releasing the grip on a form that was already gone, accepting the uncertainty that the system actually requires in order to reorganize.
This phase is often the turning point. People who can let go tend to move through. People who keep trying to reassemble what was tend to get stuck in extended depression, anxiety, or a kind of half-life that goes on for years.
Rebirth. A new configuration emerges. Not the old one, recovered. Something different — usually wiser, often more whole, sometimes more useful. The person who comes through is recognizably the same person, but reorganized. The values may be different. The priorities have shifted. What used to matter doesn't, and what didn't seem to matter now does.
This isn't a fairy tale ending. The new configuration will eventually become its own form of stability, which will eventually meet its own disruption, and the cycle will turn again. But for now, something has been completed. The transformation that wanted to happen has happened.
Why This Shape Is Everywhere
The reason this same arc shows up across mythology, therapy, contemplative practice, and storytelling isn't coincidence. It's because the arc describes how change actually works in any complex living system.
Living systems can't transform continuously. They have to organize themselves into coherent forms in order to function. But the forms they organize themselves into eventually become limiting — too rigid, too narrow, too poorly matched to a world that keeps changing. At some point, the system needs to reorganize.
Reorganization requires a period of disorder. You can't go from one coherent form to another without passing through some loss of coherence. The old form has to dissolve before the new one can take shape. This is true of biological systems, of relationships, of cultures, of nervous systems, of psychological structures.
The descent phase, in this picture, isn't a malfunction. It's a feature. It's the necessary period of disorder that allows new order to emerge. Without it, the system can't actually change. It can only repeat itself with cosmetic variation.
This is why stories that don't have a real descent feel hollow. The protagonist who solves their problem without actually being undone by it hasn't transformed; they've just rearranged the furniture of an unchanged self. The stories that move us are the ones where the protagonist genuinely loses something, genuinely falls into uncertainty, and genuinely emerges different. We recognize the shape because we know it, even when we haven't named it.
What This Means Clinically
For people in the middle of this arc, naming it can be one of the most useful interventions there is.
The depression that arrived after the divorce isn't necessarily a diagnosis. It might be the descent phase of a transformation. The disorientation that's followed a major loss isn't necessarily a malfunction. It might be the necessary disorder that allows reorganization. The fear during a psychedelic experience that something is dissolving isn't necessarily a bad sign. It might be exactly what needs to happen for the experience to do its work.
This doesn't mean every difficult period is automatically a transformation. Sometimes depression is just depression and needs treatment. Sometimes anxiety is just anxiety and needs care. Not every dark phase has a redemptive arc.
But many of the long, painful, disorienting phases people live through are transformations in progress, and the cultural script — something is wrong with you, fix it, get back to normal as quickly as possible — actively interferes with the work the system is trying to do.
What helps, in these phases, isn't usually fixing. It's holding. The slow steady company of someone who can witness the descent without panicking, without trying to rescue, without insisting on a faster timeline than the system can support. The therapist who can sit with the dissolution. The friend who can be present without needing to fix. The contemplative practice that honors the disorder rather than fighting it. The relationship that doesn't end when one person stops being who they were.
This is part of why depth-oriented therapy works the way it does. It doesn't try to shortcut the descent. It supports the system through what the system needs to do, at the pace the system can sustain.
What This Means for Psychedelic Work
This arc has particular relevance for psychedelic experience.
A well-prepared psychedelic experience often produces, in compressed form, the same shape that life-scale transformations produce over years. The medicine softens the existing structure. The person passes through some form of descent — often involving fear, grief, or the dissolution of familiar identity. There's a moment of letting go. And something new comes into view.
This is why psychedelic experiences feel transformative — not because they install new beliefs or produce new insights, but because they put the person through a compressed version of the actual arc of change. The system gets to do, in a few hours, what would otherwise take years.
The risk is that without preparation and integration, the arc gets cut short. The descent gets framed as a bad trip. The letting go doesn't quite happen. The rebirth doesn't consolidate because there's no infrastructure of life to support it. The medicine produced the conditions for transformation; the surrounding work needed to support it didn't happen.
This is part of why integration is so important. The arc has to be allowed to complete. The new configuration that emerged during the experience needs sustained support to take root in ordinary life. Without that, the person glimpsed something but didn't become someone who can live it.
What This Looks Like When You're In It
If you're reading this and recognizing yourself in the descent — the disorientation, the loss of clear identity, the sense that what worked isn't working anymore — there are a few things worth holding.
This phase is harder when you fight it. The cultural script will tell you that you should be productive again by now, that you should have figured it out, that the disorientation is a problem to solve. Letting these messages drive you tends to keep you in the descent longer, not less long.
Real support helps. Not the kind of support that tries to talk you out of where you are, but the kind that can witness it. A therapist who understands transformation. A friend who can be present without needing to fix. A contemplative practice that gives the disorder a container.
Slowing down often helps. The descent often coincides with a slowing of energy, motivation, and clarity. This isn't laziness. It's often the system pulling resources inward for the reorganization work that's happening underneath. The activity that the old self had been sustaining isn't quite available anymore, and trying to maintain it can make the whole process longer.
The body needs more, not less. Sleep, food, movement, time outside, time with people who care about you. The reorganization is happening in your nervous system, in your body. Treating yourself with care during this phase isn't indulgence. It's part of how the system actually does the work.
And the descent does end. Not always when you want it to. Not always how you expect. But the arc has a shape, and the descent is not the destination. Something new is trying to form. Your job, much of the time, is to allow the formation to happen at the pace it can happen — and to not abandon yourself while it does.
A Closing Reflection
What I find most useful about this arc, both clinically and personally, is what it suggests about what change actually requires.
We tend to want growth without descent. Transformation without loss. New configurations without the disorder of the old one dissolving. The cultural fantasy is of continuous, painless improvement — a self that keeps getting better in a straight upward line.
The actual shape of change doesn't work that way. The systems that transform are the ones that pass through periods of disorder. The selves that genuinely become more whole are the ones who let the old self come undone. The lives that deepen are the ones that include real descent, not just rearrangement.
This isn't a counsel of despair. It's the opposite. It means that what feels like falling apart is often the necessary phase of becoming. The moments that look like failure, from inside, are often the system doing exactly what it needs to do.
If you're in one of those moments now, you are not broken. You are not failing. You are not going backward. You may be exactly where you need to be, doing exactly what the next configuration of your life requires.
If you'd like a place to be held through that work — through depth-oriented therapy, integration support, or contemplative practice — you're welcome to book a consultation.
A Recommended Watch: Unraveling the Dream
A new documentary from the Waking Up app, executive produced by Sam Harris and featuring Anil Seth, Robin Carhart-Harris, and Shamil Chandaria, makes a clinically important distinction: psychedelic experiences produce states, but contemplative practice produces traits — and traits are what actually change a life. A therapist's brief recommendation and a note on what the distinction means for integration.
There's a film I'd recommend if you're sitting with questions about consciousness, psychedelics, meditation, or what these conversations have to do with each other.
It's called Unraveling the Dream: Psychedelics, Awakening, and the Brain. Released in April 2026, directed by Jake Orthwein, executive produced by Sam Harris and Jaron Lowenstein, and produced by the Waking Up meditation app. It runs about an hour and is freely available on YouTube.
The film traces a single thread that I think more people need to encounter. It starts with Aldous Huxley's 1953 mescaline experiment — the experience that produced The Doors of Perception and seeded most of what came after in Western psychedelic culture. From there it moves through the contemporary neuroscience of consciousness, drawing on interviews with three of the most important thinkers in the field: Anil Seth, Robin Carhart-Harris, and Shamil Chandaria.
What makes the film unusual is that it doesn't quite fit either of the standard genres of psychedelic content. It isn't an enthusiast piece selling the medicines as the next mental health revolution. It also isn't a cautionary takedown. It sits in a more honest place, and the question it ends with is one I find clinically important.
What the Film Actually Argues
The central insight, developed across the film's hour, is a distinction that's easy to miss in most psychedelic conversation.
Psychedelic experiences can produce profound states. The boundaries of the self loosen. Ordinary perception becomes vivid in ways that feel revelatory. Material that ordinarily sits beyond conscious reach can come into view. For many people, these experiences are among the most significant of their lives.
But a state is a temporary thing. It happens, and then it ends. The brain returns, mostly, to its baseline configuration. The patterns that produced the suffering in the first place reassert themselves. And the person is left with the memory of having glimpsed something — without necessarily having become someone who can live it.
The film's argument, drawing on the contemplative tradition that Waking Up represents, is that traits are what actually change a life. Not states. Traits — durable changes in how the underlying system organizes itself, built over time through repeated practice — are what last. And the practice that builds them is, in this view, primarily contemplative.
Or, in the film's framing: destroying the ego is a chemical event that lasts four to six hours. Transcending it is a skill, and developing that skill is the work of years.
Why This Distinction Matters Clinically
I see this constantly in clinical work.
People come back from powerful psychedelic experiences with vivid memories of what they encountered, sometimes with sustained behavioral changes for weeks or months, and then often with a gradual return of the patterns that brought them to the medicine in the first place. The state was real. The change it produced was real, while it lasted. But without something that helps the underlying configuration of the mind actually shift, the door that opened tends to close.
This is part of what good integration work is for, and part of what's missing in much of the current commercial psychedelic landscape. The medicine alone, even when it produces profound experiences, doesn't reliably produce lasting trait change. What seems to matter more is what happens afterward — the slow work of bringing what was glimpsed into the structure of ordinary life.
For some people, this happens through ongoing contemplative practice. Daily meditation, in particular, appears to be one of the most reliable ways of consolidating the openness that a psychedelic experience can briefly produce. The medicine shows you something; the practice helps you slowly become someone who can hold what you saw, not as a memory of a peak experience but as a present-tense quality of how you live.
For others, it happens through depth-oriented therapy that takes the experience seriously and works with it over time. For others, through community, ritual, or other forms of sustained practice. The form matters less than the underlying fact: states are not enough on their own, and traits are what allow real life to actually shift.
What I'd Take From the Film
A few things the film does well that I think are worth sitting with:
It's honest about the limits of psychedelic experience. It doesn't suggest that the medicines fix anything on their own, and it explicitly points to the work that has to surround them for the openings they produce to actually take root.
It's grounded in the actual neuroscience, with serious interviews rather than dramatic claims. Seth on consciousness as construction. Carhart-Harris on the entropic brain. Chandaria on the bridge to contemplative tradition. The interviews give you something substantive to think with.
And it asks the right closing question — not should you take psychedelics, but what kind of practice would let you actually live the freedom these experiences can sometimes glimpse?
That question is, I think, the most important one to bring out of any encounter with psychedelic experience, whether you're considering one or integrating one you've already had. The medicine, when it works, opens a door. What you do with the open door is where the actual change lives.
Where to Watch
The film is freely available on YouTube on the Waking Up channel. The link is here. It's about an hour, and worth setting aside the time rather than half-watching.
If you find yourself moved by the questions it raises — about meditation, integration, or what serious work with these experiences could look like for you — you're welcome to book a consultation.
How Consciousness Emerges Through the Body
Consciousness isn't produced by the brain in isolation — it emerges continuously from the conversation between brain, body, and environment, with interoception and proprioception as constitutive elements of experience itself. A therapist on what this picture means for healing, for psychedelic integration, and for why working only with the mind often leaves the patterns that hurt us untouched.
There's a moment that often happens in deep therapeutic work, and especially in psychedelic experience, that defies the way most of us were taught to understand the mind.
A client begins to cry — not because they were thinking sad thoughts, but because something has begun to release in their chest, their throat, their belly. The tears come from somewhere underneath language. They don't know exactly what they're crying about. The body, in some way they hadn't been tracking, has been carrying this all along.
Or someone in the middle of a psychedelic experience suddenly understands something — not as a thought arriving in their mind, but as a felt sense moving through their whole system. The understanding is bodily before it becomes verbal. By the time they can put it into words, the words feel like a translation of something that happened in a different language.
These moments are common in depth work, and they point at something the dominant Western model of consciousness has long had trouble accommodating: that the body isn't a vehicle the mind rides around in. The body is part of how the mind happens. Consciousness isn't located somewhere inside your skull; it's something that emerges, continuously, from the ongoing conversation between brain, body, and world.
This isn't mysticism. It's increasingly the conclusion of contemporary neuroscience. And a 2015 paper in Frontiers in Psychology by Payne, Levine, and Crane-Godreau — Somatic Experiencing: using interoception and proprioception as core elements of trauma therapy — articulates one of the clearest applications of this picture to the question of how healing actually works.
I want to walk through this carefully, because it underlies a great deal of what makes Path of the Pearl's approach distinct — and because it explains why psychedelic experience, and the integration work that follows, has to reach the body if it's going to reach anything that lasts.
The Old Picture and Its Limits
For most of the twentieth century, the dominant model treated the brain as an information processor. Sensory data comes in, gets analyzed, and conscious experience is the output. The body shows up in this picture as a delivery system for sensory input and a recipient of motor commands, but the consciousness itself happens in the brain.
This model has been productive scientifically. It also has serious limits that have become harder to ignore.
It struggles to explain why bodily states so reliably alter mental ones. Why slow breathing genuinely calms anxiety in ways that thinking about being calm doesn't. Why posture affects mood, why hunger affects judgment, why fatigue changes what you believe about your life. The brain-as-isolated-processor model treats these as side effects. The lived experience suggests they're closer to the main event.
It also struggles with phenomena that contemplative and somatic traditions have known about forever. Why moving the body changes the mind. Why breath work reliably produces shifts in consciousness. Why people who carry trauma in their bodies often can't be reached through talk alone, and why those who learn to listen to the body can sometimes access material that conversation never quite touches.
The newer view that's emerging across cognitive science is what's sometimes called embodied cognition or embodied consciousness. The premise is straightforward: the brain, the body, and the environment aren't three separate systems that occasionally interact. They're one continuous system, and what we call consciousness is what that system does.
The Inside View: Interoception
One of the most important pieces of this picture is interoception — your brain's ongoing perception of the internal state of your body.
You don't usually think about interoception explicitly, but it's running constantly underneath your conscious experience. Your brain is continuously tracking signals from inside you: heartbeat, breath, gut sensations, muscle tension, blood pressure, temperature, the subtle felt sense of being a body. These signals aren't background noise. They're constitutive of how you feel, what you notice, and even what you think.
When you're anxious, much of what you experience as anxiety is interoceptive — your awareness of your racing heart, your tight chest, your shallow breath. When you're calm, interoception reports something different — slower heart, deeper breath, softer belly. The thoughts that arise on top of these states tend to match them. Anxious bodies produce anxious thoughts. Calm bodies produce calmer thoughts. The direction of causation runs both ways, but interoception is doing far more of the work in shaping experience than most people recognize.
This is why directly working with the body's internal state often changes what's happening psychologically faster than working with the thoughts. Slow your breath, and the anxious cognitions begin to soften — not because you've talked yourself out of them, but because the interoceptive substrate that was generating them has shifted.
It's also why, for people whose interoceptive signal has been disrupted — which is common in trauma — the work of healing involves rebuilding access to the body's inner life. When the connection between conscious awareness and bodily sensation has been severed, the system loses one of its most important regulatory tools. Restoring that connection, slowly, is often a central piece of trauma therapy.
The Outside View: Proprioception and Movement
There's a second layer too: proprioception — your sense of where your body is in space, how it's positioned, how it's moving.
Like interoception, proprioception runs continuously and mostly outside conscious awareness. You don't have to think about where your hand is; you just know. You don't have to direct each step; you walk. The proprioceptive system is what allows the body to move through the world without constant deliberate guidance.
What's interesting clinically is that proprioception, like interoception, is bidirectional. Moving your body changes your mental state in measurable ways. The slow, careful movement of yoga or qi gong doesn't just feel good — it actually shifts the brain's processing patterns. The rhythmic movement of walking has been shown to facilitate emotional integration in ways that sitting still doesn't. The forms of movement traditional cultures have used for healing for thousands of years — dance, ritual movement, ceremony — engage the proprioceptive system in ways that produce real psychological change.
The Payne, Levine, and Crane-Godreau paper specifically focuses on how interoception and proprioception together form the foundation of somatic approaches to trauma healing. Both are routes into the system where so much of suffering actually lives. Both can be trained, refined, and used as instruments of healing in ways that purely cognitive approaches can't replicate.
The Self as Embodied Process
If consciousness is genuinely embodied, then the self is too.
The felt sense of being you — the experience of being a continuous person across time, the sense of being inside your own life — isn't generated by some isolated process in the brain. It's constructed continuously from the integration of bodily signals, sensory input, memory, and the ongoing experience of being a particular animal moving through a particular world.
This means the self isn't quite the fixed thing we usually experience it as. It's a process. Your self right now is being generated, in real time, by your nervous system's interpretation of your body's current state in your current environment. Change the body's state significantly enough, and the self changes too.
This is why posture, movement, breath, and physical state can shift identity in ways that surprise us. The exhausted self at the end of a hard day is genuinely a different self than the rested one. The anxious, contracted self in fight-or-flight isn't who you are in any deeper sense — it's who your nervous system is configured as right now, and reconfiguring the nervous system reconfigures the self.
This perspective also helps make sense of what people often experience in psychedelic states and deep meditative practice. The felt sense of self can become much more obviously a construction during these states, sometimes loosening in ways that reveal its underlying mechanisms. People come back from such experiences with a different relationship to their own identity — not because they've stopped being themselves, but because they've seen, directly, how their self is being produced, moment to moment, from the underlying system.
Why This Matters for Psychedelic Work
This whole picture is foundational to why psychedelic-assisted therapy and integration work has to reach the body, not just the mind.
Psychedelics produce profound shifts in interoceptive and proprioceptive experience. The boundaries of the body become more fluid. Internal sensations become more vivid. The felt sense of being a self gets reorganized at the level of the bodily substrate that ordinarily produces it.
What this means clinically is that what's happening during a psychedelic experience is not primarily intellectual. It's somatic. The insights that arise — even the ones that feel like cognitive realizations — often emerge from bodily reorganization that's happening underneath. The work of integration, then, has to honor this. You can't fully integrate a psychedelic experience through talk alone, any more than you can fully integrate any deep experience through talk alone. The body that participated in the experience has to participate in the integration.
This is why the most thoughtful psychedelic practitioners pair the medicine work with somatic approaches. Somatic Experiencing. Internal Family Systems with attention to body sensation. Hakomi. Touch-informed work where appropriate. Breath work. Movement practices. Body-aware mindfulness. The medicine opens something; the somatic work helps the opening land in the body where it can actually take root.
Without this dimension, psychedelic experiences can produce strong cognitive impressions that fade as the brain returns to its baseline patterns. With it, the same experiences can produce lasting changes in how the person inhabits their body and their life.
Why This Matters for All Healing
Even beyond psychedelic work, this picture has implications for how to think about healing more broadly.
Many of the people I work with come in expecting therapy to be about understanding. Identify the pattern. Trace it to its origin. Develop better strategies. This is part of what therapy does, and it matters. But by itself, it often doesn't reach where the patterns actually live.
The anxiety that runs through your day isn't only in your thoughts. It's in your shoulders. In your breath. In your gut. In the way you hold yourself when you enter a room. The depression isn't only in your beliefs about life. It's in the heaviness of your body, the slowed metabolism, the way movement has dropped out of your days. The trauma isn't only in your memories. It's in the bracing pattern your nervous system has carried for decades.
Working only with the mind, while leaving the body untouched, often produces a partial change. You understand more, but the underlying state remains. The patterns return because the substrate that generates them is still configured to generate them.
The work that produces lasting change usually involves both. The cognitive understanding and the embodied reorganization. The new perspective and the new way of breathing. The processed memory and the released tension that was holding it.
Good therapy at depth, regardless of whether it involves any psychedelic medicine, attends to the body throughout. It tracks the breath. It notices what's happening in the chest, the throat, the belly. It treats the body as a participant in the conversation, not just a vehicle delivering the client to the chair.
What This Looks Like in Practice
A few small practices that honor this picture:
Before any conversation, check in with your body. What's the felt sense in your chest right now? Your stomach? Your shoulders? Most of us walk through our days without doing this even once. The thirty seconds of attention can change what's available in the next hour.
Notice the body's signals during difficult moments. When you're activated — angry, anxious, defensive — the body is usually doing something specific. Tightening, holding, bracing. Noticing it without trying to change it is itself a regulatory act. You're bringing the body into the conscious system, and that alone often shifts something.
Move when you're stuck. When thinking has become circular and unproductive, the body often holds the next step. A walk. Stretching. Slow breathing. Lying on the floor for ten minutes. The thinking mind will tell you it's a distraction. Sometimes it's the opposite — the thinking is the distraction from what the body is trying to tell you.
Take seriously what your body knows. The felt sense that something isn't right, even when you can't say why. The somatic relief when something resolves. The tension that arises around certain people, places, or topics. These aren't unreliable. They're often more accurate than the thoughts that try to override them.
Consider somatic approaches when patterns won't shift. If you've done years of therapy and certain patterns still grip you, the missing piece may be at the level of the body. Somatic Experiencing, Hakomi, Sensorimotor Psychotherapy, somatic IFS, and breath-based practices can reach places that cognitive work alone hasn't quite touched.
A Closing Reflection
The Western philosophical tradition, going back to Descartes, treated the mind and body as separate substances. I think, therefore I am — the thinking is the self; the body is something else. This split has shaped medicine, psychology, and culture for centuries.
The contemporary picture that's emerging — from neuroscience, from contemplative traditions, from somatic therapy, and now increasingly from psychedelic research — points in a different direction. The mind and body aren't separate. They're aspects of one living process. What you experience as your mind is what your whole organism is doing, in interaction with the world it lives in.
This isn't a loss of the mind's importance. It's a recovery of something the body always knew. The animal you are has wisdom that the thinking mind doesn't have direct access to. Healing — and especially the kind of deep, lasting change that psychedelic and depth work aim toward — involves rebuilding the conversation between these two aspects of yourself.
The body has been participating in your life the whole time. The question is whether the conscious mind will start listening.
If you'd like to explore depth-oriented work that takes the body seriously — whether through somatic therapy, integration support for past or future psychedelic experiences, or contemplative practice — you're welcome to book a consultation.
The Missing Piece in Psychedelic Therapy: How We Make Meaning of What We Experience
When people have profound psychedelic experiences, they often emerge with spiritual, existential, religious, and theological questions that current clinical models aren't well-equipped to address. A therapist on a 2023 JAMA Psychiatry paper arguing that the meaning-making dimension of psychedelic therapy isn't peripheral but central — and what taking it seriously would actually require.
There's a strange omission in much of the clinical literature on psychedelic therapy.
The research papers will tell you about neuroplasticity, about serotonin receptors, about the default mode network and predictive processing. They'll describe the symptom changes — depression scores dropping, anxiety subscales improving, addiction patterns loosening. The mechanism gets traced through brain imaging, neurotransmitter activity, network dynamics.
What they often don't address is what people actually experience.
Not the activated receptors. The sense of having met God, or having understood the universe, or having encountered a deceased grandmother, or having recognized that everything is connected, or having confronted their own mortality, or having seen, in a way they can't put into words, what their life is for. These aren't side effects of the medicine. For many people, they are the heart of what happened.
A 2023 paper in JAMA Psychiatry, Importance of Integrating Spiritual, Existential, Religious, and Theological Components in Psychedelic-Assisted Therapies, addresses this gap directly. The authors — Palitsky, Kaplan, Peacock, and colleagues — argue that the spiritual, existential, religious, and theological dimensions of psychedelic experience are not peripheral. They may be central to how healing actually happens. And current clinical models, by failing to systematically address them, are leaving a significant part of the work undone.
I want to walk through this carefully, because I think the paper is naming something that matters enormously for the future of psychedelic therapy — and for the broader question of what any depth-oriented therapy is actually for.
What Most Clinical Models Miss
Modern psychedelic therapy follows a three-phase structure: preparation, the experience itself, and integration. Within each phase, there's usually careful attention to safety, screening, expectation-setting, emotional support, and basic therapeutic principles.
What's often missing is a framework for working with the meaning-making that almost inevitably arises.
People emerge from psychedelic experiences having encountered material that doesn't fit neatly into clinical categories. I felt like I was dying, and it was okay. I saw what I came here to do. I forgave my mother in a way I never thought possible. I understood, for those hours, that love is the actual fabric of reality. I met a presence I can only call sacred.
These aren't symptoms to be managed. They're not delusions to be corrected. They're not metaphors to be translated into psychological terms. They are the substance of the experience for many people, and the work of integration involves figuring out what to do with them.
But the clinical models rarely address how. Most psychedelic therapy training, even in established programs, treats spiritual and existential material as something the therapist is expected to navigate intuitively, without formal preparation. Some therapists handle this well. Many handle it poorly — either dismissing the meaning-making as epiphenomenal, or unwittingly imposing their own metaphysical assumptions, or simply not knowing what to do when a patient describes experiences that exceed the framework they were trained in.
The JAMA paper proposes that this needs to change. Not because every patient is spiritual or religious, but because all patients are meaning-making creatures, and psychedelic experiences amplify exactly the dimensions of life where meaning is most actively constructed.
The SERT Framework
The paper organizes these dimensions into four overlapping domains, captured by the acronym SERT:
Spiritual — the felt sense of connection to something larger, sacred, or deeply meaningful. This doesn't require any particular belief system. Atheists, agnostics, and people of all religious traditions can have spiritual experiences in this sense.
Existential — the human confrontation with mortality, meaning, identity, freedom, and the basic conditions of existence. The questions that arise when ordinary distraction falls away and life's underlying realities become unavoidable.
Religious — the structured belief systems, communal practices, and cultural traditions through which many people have historically organized spiritual and existential experience. Religion provides language, ritual, and community for what would otherwise be entirely private.
Theological — the more developed attempts to articulate the nature of ultimate reality, the divine, and the structures that might lie beneath ordinary experience. The intellectual and philosophical work of trying to make sense of what's been encountered.
These four domains aren't separate compartments. They overlap and inform each other. Together, they describe the dimension of human life where deep meaning is made — the same dimension that psychedelic experiences so often touch directly.
What the paper argues is that clinical work with psychedelic experience that ignores all four of these dimensions isn't neutral. It's incomplete. And incomplete care, in vulnerable states, can do harm.
What Happens Without This Framework
Without a framework for meaning-making, several predictable problems emerge in psychedelic therapy.
Patients get left alone with experiences they can't make sense of. Someone has a profound mystical encounter during a session. They leave wanting to talk about it. The therapist, lacking framework or training, redirects toward symptom management or cognitive integration. The experience gets quietly sidelined. The patient is left to figure out what it meant on their own, often without the contemplative or theological resources to do this well.
Therapists impose their own beliefs. A therapist with no formal training in spiritual care will inevitably bring their own assumptions into the room. A secular materialist therapist may unconsciously communicate that the patient's mystical experience was just their brain doing something. A spiritually inclined therapist may encourage interpretations that align with their own beliefs. Neither is neutral. Both can shape, sometimes coercively, what the patient comes to believe about their own experience.
Patients with religious frameworks get inadequate support. A devout Christian who has a psychedelic experience that doesn't fit her theology may feel deeply disoriented. A Jewish patient who encounters something that feels like the divine may need to integrate that within his existing spiritual life. Many clinical settings have no infrastructure for engaging with these specific religious frameworks, even though the patient's religious life is often centrally relevant to how they'll integrate the experience.
Atheists and secular patients get inadequate support too. A secular patient may have an experience that destabilizes their worldview. They emerge convinced of things they didn't believe before. Without help, they may either uncritically adopt new metaphysical commitments or repress what they experienced because it doesn't fit their existing framework. Either response leaves the integration incomplete.
Spiritual distress goes unaddressed. Not all psychedelic experiences are positive. Some involve profound existential distress — feeling abandoned by God, encountering darkness that doesn't resolve, losing a faith that previously felt secure, confronting mortality in ways that produce lasting fear. Clinicians without training in spiritual care often don't recognize these as the spiritual emergencies they are, and the patient is left without adequate support.
The paper documents that all of these problems are common in current psychedelic therapy. They're not edge cases. They're routine consequences of clinical models that treat meaning-making as someone else's problem.
Why Psychedelics Specifically Amplify This Need
There's a specific reason this matters more in psychedelic therapy than in many other forms of clinical work.
Psychedelics, neurologically, increase what researchers call cognitive flexibility and suggestibility. The rigid filters through which we ordinarily organize experience loosen. New patterns can form. Existing patterns can be revised.
This is part of what makes the medicines therapeutically valuable. It's also what makes them ethically demanding. In a state of increased suggestibility, what the patient is exposed to — including what the therapist says, what the music suggests, what the cultural context implies, what the patient already half-believed — has unusual influence. The window in which new meaning gets made is unusually wide.
For meaning-making specifically, this matters enormously. The interpretations a patient forms during and immediately after a psychedelic experience often consolidate into how they'll understand the experience long-term. If those interpretations are guided thoughtfully, with attention to the patient's own values and tradition, integration tends to go well. If they're guided poorly, or not guided at all, the patient may end up with conclusions that don't serve them — sometimes with effects that persist for years.
This is part of why psychedelic therapy isn't just pharmacology. It's a kind of clinical work where the meaning context the therapist creates is itself part of the medicine. Or, when handled badly, part of the harm.
The Particular Difficulty for Therapists
I want to be honest about how difficult this is from the therapist's side.
Most therapists are trained, appropriately, in maintaining a kind of neutrality about patients' spiritual and existential lives. We're taught not to impose our own beliefs, not to evaluate the truth of religious convictions, not to direct patients toward particular metaphysical conclusions. This neutrality serves patients well in most clinical settings.
But psychedelic therapy challenges this stance in specific ways. Patients in altered states are bringing material that requires engagement. They're often asking, sometimes directly, what their therapist makes of what just happened. They want to know if it was real. They want to know what to do with it. They want help making sense of an experience that doesn't fit easily into their existing frameworks.
A therapist who maintains complete neutrality in this context can come across as dismissive or absent. A therapist who engages without care can impose. Finding the middle path — being substantively present without becoming directive — requires both training and personal preparation that most current programs don't adequately provide.
The paper's recommendation is that psychedelic-assisted therapy programs need to systematically include training in spiritual and existential care. Not turning therapists into chaplains or spiritual directors, but giving them the tools to recognize when these dimensions are active, to support patients in their own meaning-making rather than imposing the therapist's, and to refer or consult when more specific religious or spiritual expertise is needed.
How This Might Look in Practice
What would good integration of meaning-making look like in psychedelic therapy?
A few possibilities, drawn from the paper and from clinical practice:
Preparation that includes meaning. Before the session, exploring with patients what meaning systems they already work within. What gives their life meaning now? What spiritual or religious frameworks have shaped them? What existential questions have they been sitting with? What would they like to be open to during the experience? This gives the therapist a sense of the patient's existing meaning architecture, which helps the integration that comes later.
Non-directive presence during the experience. Skilled facilitators learn to support whatever arises without steering it toward particular interpretations. Notice what's here. Be with what comes. Let it move you wherever it wants to move you. The work isn't to install meaning; it's to make space for the patient's own meaning to emerge.
Integration that honors the meaning as well as the symptoms. After the experience, integration sessions should make explicit room for the spiritual and existential material, not just the psychological. What did you experience that felt sacred? What questions does this raise for you about your life? Has anything shifted in how you understand your purpose, your relationships, your mortality? These are integration questions, not just clinical ones.
Referral and consultation when needed. Therapists shouldn't be expected to be experts in every religious tradition, every theological framework, every philosophical system. Building referral networks with chaplains, spiritual directors, religious teachers, and contemplative practitioners — who can be consulted as appropriate to the patient's tradition — should be part of good psychedelic therapy infrastructure.
Honest acknowledgment of the limits. A therapist isn't a theologian or a spiritual teacher. Being clear about what the therapist can and cannot offer, and supporting patients in finding the right resources for the meaning-making questions they're sitting with, is itself part of responsible care.
A Wider Lens
What I find most clinically valuable about the JAMA paper is something its authors only touch on implicitly: this isn't really a problem specific to psychedelic therapy.
It's a problem in most contemporary mental health care.
For most of the 20th century, clinical psychology distanced itself from religious and spiritual frameworks as a way of establishing itself as a serious science. The cost was that the meaning-making dimension of human life — the dimension where mortality, purpose, identity, and the sacred live — got increasingly handed off to people who weren't psychologically trained, or simply got ignored.
This worked, sort of, in eras when most patients had robust religious frameworks of their own. People could do the meaning-making outside therapy — in church, in community, in the structured rituals of their tradition. Therapy could focus on the psychological without addressing the existential, because the existential was being addressed elsewhere.
That arrangement has been quietly breaking down for decades. Many of my patients don't have religious frameworks they're embedded in. Many were raised in traditions they've left and haven't replaced. Many are spiritually serious but unaffiliated. Many are atheists or agnostics for whom existential questions remain real even without a religious context. The meaning-making dimension of their lives has nowhere external to land. It's all happening inside, often unsupported, often in the form of low-grade chronic distress that gets called depression or anxiety because we don't have better language for it.
This is part of why so many people are turning toward psychedelic therapy, contemplative practice, indigenous traditions, and other forms of meaning-making that the mainstream mental health system hasn't been able to provide. Not because traditional therapy is failing on its own terms, but because the existential dimensions of suffering aren't being addressed anywhere, and people are starving for them.
What the JAMA paper is naming, specifically about psychedelic therapy, is a broader truth: good care of human suffering eventually has to include the meaning-making dimension. The depression isn't only chemical. The anxiety isn't only cognitive. The grief isn't only emotional. Underneath, in most of the people I see, are existential and spiritual questions that need to be honored, examined, and supported.
What This Means for Path of the Pearl's Work
This is part of why I work the way I do.
Path of the Pearl is anticipating a future in which psilocybin and other psychedelic medicines will be legally available for therapeutic use in California. The technical aspects of that work — preparation, safety, dose, integration — matter enormously. But they're not the whole picture.
The deeper work, in my view, is creating clinical space where the spiritual, existential, and meaning-making dimensions of psychedelic experience can be held with care. Not by imposing any particular framework. Not by claiming expertise in any patient's specific tradition. But by recognizing that these dimensions are active in almost every meaningful psychedelic experience, by being able to sit with them without flinching or directing, and by helping each patient find their own way through what's been opened.
This requires training beyond standard clinical psychology. It requires the therapist's own contemplative and existential work. It requires building relationships with chaplains, spiritual directors, and teachers across traditions who can be consulted appropriately. It requires honesty about the limits of what any one practitioner can offer.
For me, this isn't a separate add-on to clinical work. It's part of what depth-oriented therapy has always been about, made more visible by the demands of working with psychedelic experiences. The same questions that arise vividly under the medicine — what is my life for? what happens when I die? what is sacred? who am I underneath the story I've been telling? — are quietly present in most of the work I do, whether or not any medicine is involved.
A Closing Reflection
The JAMA paper's central argument is, in a way, an old one dressed in clinical language. Healing is not just biological. It's not even just psychological. It's also about how we make sense of being alive — what we take to be sacred, what we believe gives our lives meaning, how we understand our place in the larger reality we're part of.
For thousands of years, traditional cultures have known this. The healing arts were embedded in larger frameworks of meaning — religious, communal, ceremonial. Modern Western medicine separated the biological from the spiritual for good reasons, but at a cost.
Psychedelic therapy is, in some sense, forcing the conversation back to where it needs to be. The medicines produce experiences that won't fit into purely biological or psychological frameworks. They demand to be addressed at the level where meaning is made. Clinicians who try to work with these medicines while avoiding the meaning-making dimension are increasingly recognizing that they can't.
This is hopeful, I think. Not because it means we're returning to pre-modern frameworks, but because we're being asked to develop new ones — frameworks that take both science and meaning seriously, that honor both the brain and the soul, that can hold both the patient's symptoms and their deepest questions.
The work is just beginning. The current clinical models are inadequate to it. But the direction is clear, and the resources — from contemplative traditions, from existential psychology, from interfaith chaplaincy, from indigenous wisdom traditions — are available. The question is whether the field can grow into them.
If you'd like to explore what depth-oriented work that honors the meaning-making dimension might look like for you, you're welcome to book a consultation.
Can Psychedelics Reveal Truth, or Just Change Your Mind?
When someone has a profound psychedelic experience and emerges with strong convictions about the nature of reality, what should they do with those convictions? A therapist on philosopher Chris Letheby's careful argument that psychedelic experiences can produce genuine insight — particularly into the constructed nature of the self — without requiring the metaphysical claims that often accompany them.
There's a particular kind of conversation that happens in the weeks and months after a powerful psychedelic experience.
The person who has had the experience returns from it changed. They've seen something. Felt something. Understood something. They want to talk about it, and as they try, they find themselves making claims that sound, in ordinary daylight, somewhere between profound and embarrassing. I understood the nature of reality. I encountered God. I saw that everything is connected. I learned that death isn't real. I knew, for those hours, exactly what the universe is.
The listener — even a sympathetic one — often doesn't know what to do with these reports. The experience clearly mattered. The person clearly isn't lying. Something happened that they're trying to convey. But the claims being made about reality itself often go further than what any experience, however powerful, could actually justify.
This is one of the most important questions in psychedelic medicine, and it's underaddressed in most popular conversation about the field. When someone has a profound psychedelic experience and emerges with strong convictions about the nature of reality — convictions they didn't have before, convictions that feel utterly certain — what should they do with those convictions? Are they genuine insights into something deeper? Or are they powerful experiences that the brain is producing for its own reasons, with no special access to truth?
The philosopher Chris Letheby has written one of the most important books on exactly this question. His Philosophy of Psychedelics, published by Oxford University Press in 2021, takes the philosophical questions about these experiences as seriously as the clinical and neurological ones. His answer is more interesting than either pole of the usual debate, and I think it's clinically essential for anyone considering or integrating psychedelic experiences.
The Two Camps and Why Both Are Incomplete
The conversation about psychedelics tends to polarize between two positions.
The mystical view treats psychedelic experiences as windows onto deeper reality. Ego dissolution reveals the true nature of the self. Mystical experiences are encounters with something genuinely transcendent. The medicine opens doors that ordinary consciousness keeps closed. This view has deep roots — in indigenous traditions, in 1960s thinkers like Aldous Huxley, in much contemporary spiritual psychedelic culture. It honors the felt depth of these experiences and treats them with the seriousness they often demand.
The naturalistic view treats psychedelic experiences as brain events. Powerful, sometimes useful, but ultimately just neurochemistry. The sense of cosmic significance is a side effect of altered brain function. The mystical content isn't real; it's a particularly compelling form of hallucination. This view honors scientific caution and refuses to make claims that can't be empirically supported. It also tends, in its blunter forms, to dismiss what people have actually experienced as somewhere between delusion and chemistry.
Both views miss something. The mystical view risks unjustified metaphysical claims. The naturalistic view risks dismissing experiences that genuinely matter and have measurable therapeutic effects.
Letheby's project is to find a third position. His argument, in essence: psychedelic experiences can produce real epistemic value — genuine insights, real knowledge — even if we don't accept their metaphysical claims at face value. You can take these experiences seriously without taking them literally.
The Comforting Delusion Objection
Letheby starts with what he calls the Comforting Delusion Objection. It's the worry that psychedelic therapy might be working only by deluding people with false metaphysical beliefs — that the depression lifts because the person now believes the universe loves them, or that they've encountered God, or that death isn't real. If that's how the therapy works, the objection goes, then it's working through deception, and that's ethically problematic even if it relieves suffering.
This objection deserves to be taken seriously. If psychedelic therapy primarily produced relief by installing false beliefs, it would have a real ethical problem. The therapist would be implicated in a kind of psychological con — even a well-meaning, helpful con, but still one whose mechanism depends on deceiving the patient.
Letheby's response is methodical. He argues that the therapeutic benefit of psychedelic experience doesn't actually depend on metaphysical conclusions. It depends on something else: phenomenological insight into the constructed nature of the self.
This is the key move. Let me unpack it.
What's Actually Being Revealed
When someone has a psychedelic experience of ego dissolution — when the felt sense of being a separate, continuous self temporarily loosens — they're not necessarily discovering anything about the metaphysical structure of the universe. They are discovering something quite specific about themselves: that the self they ordinarily experience as solid and continuous is, in fact, something constructed. Something the brain is doing. Something more flexible and less essential than it feels.
This is not a metaphysical claim. It's a claim about your own mind. And — importantly — it's almost certainly true. The neuroscience converges with the phenomenology: the self is a model the brain constructs, not a fixed entity it contains. People who experience this directly, even briefly, often emerge with a different relationship to themselves. Less identified with the suffering self. More aware that the patterns they've been running aren't permanent features of who they are. More able to consider that change is possible at a deeper level than they had imagined.
This is what Letheby calls knowledge by acquaintance — knowing something not as an abstract claim but through direct experience. A person who has never been heartbroken can know intellectually that heartbreak is painful. A person who has been heartbroken knows it in a different way. Psychedelic experience can produce knowledge of the constructed nature of the self in this richer, more directly known sense.
This kind of knowledge, Letheby argues, is real, valuable, and naturalistically respectable. You don't need to commit to any controversial metaphysical claim to acknowledge that someone who has directly experienced the constructed nature of their own self has learned something genuine.
What's Not Necessarily Revealed
The trouble comes when this insight gets extrapolated.
Many psychedelic experiences come with a sense of cosmic significance. The person doesn't just feel that their self is constructed; they feel they have understood the universe itself. Reality is consciousness. Everything is one. There is no death. We are all connected at the deepest level. I have encountered the divine.
These claims may be true. Some of them may even be true in ways philosophy can be slow to acknowledge. But they go further than the experience can actually justify. The experience produced certainty. The certainty is real. But certainty is not the same as accuracy, and Letheby is careful to point out that the very neurochemistry that produces the felt sense of profound insight may also produce overconfidence in conclusions that haven't been adequately tested.
This is one of the genuine risks of psychedelic experience that doesn't get talked about enough. The medicines don't just produce experiences. They produce conviction. The conviction can outpace the justification. People can emerge from these experiences with metaphysical beliefs they hold with the certainty of having known them directly, and they can build their lives around those beliefs in ways that don't always serve them.
I see this clinically. The person whose marriage breaks up because they've decided, after a ceremony, that their partner doesn't share their cosmic understanding. The person who quits a career they were good at to follow a calling they received during a journey. Sometimes these decisions turn out to be wise. Often, in retrospect, they look like a person acting on certainty that hadn't quite been tested against ordinary life.
The risk isn't that people have spiritual experiences. It's that they conflate the depth of an experience with the truth of every claim that emerges from it.
Letheby's Resolution
Letheby's framework offers a way through this.
The therapeutic and epistemic value of psychedelic experience, on his account, doesn't depend on the metaphysical claims being true. It depends on something more modest and more defensible: that the experiences reveal the constructed nature of the self, expand the person's sense of what's psychologically possible, and create conditions in which rigid patterns of thought and feeling can soften.
This is what produces lasting change. Not the conviction that consciousness is fundamental to the universe, or that one has encountered God. The experiential recognition that the self you've been suffering inside is not as solid as it felt. That recognition, even briefly held, can be liberating in ways that careful philosophical argument never quite is.
The metaphysical content — the sense of cosmic significance, the encounter with what may or may not be the divine — Letheby treats with what he calls epistemic humility. These experiences shouldn't be dismissed as meaningless hallucinations. They also shouldn't be treated as proof of metaphysical claims they can't independently establish. The right stance is something like: something real happened that I don't fully understand. I'll let it work on me without committing too quickly to what it means.
This is, I think, the most clinically and philosophically responsible way to hold psychedelic experience. It honors the depth without ceding judgment. It accepts the value without endorsing every claim.
Why This Matters for Integration
This question is not abstract. It comes up constantly in integration work with people who have had powerful psychedelic experiences.
The person who returns from a journey convinced of something they hadn't believed before faces a real choice. They can integrate the experience — let its depth and meaning continue to work on them — without yet committing to particular metaphysical conclusions. Or they can quickly translate the experience into beliefs and start rearranging their life around those beliefs.
The first path tends to produce more sustainable change. The depth of the experience gets honored. The harder work of letting it gradually reshape ordinary life can unfold over months and years. The metaphysical questions can stay open, considered, examined against further experience and ordinary judgment.
The second path is more vulnerable to a particular kind of trap. Beliefs adopted in the wake of profound experience are sometimes adopted to protect the experience — to preserve its meaning by codifying it. But this codification can become rigid. The person becomes someone with a particular spiritual identity, a particular metaphysical commitment, a particular way of seeing the world they're now invested in defending. The original openness that made the experience meaningful can harden into something more brittle.
This is one form of what's sometimes called spiritual bypass — using spiritual conclusions to avoid harder psychological work. The person who has decided, after a ceremony, that everything happens for a reason may use that belief to avoid grieving real losses, to bypass difficult feelings, to skip over the slow work of actually changing how they live. The metaphysical conclusion gets installed where the harder work should be happening.
Good integration work helps people stay with the experience without rushing into beliefs that might not serve them. What was true about what you experienced? What's worth letting work on you? What conclusions are you reaching that may have outrun the evidence? These are questions a thoughtful integration therapist can help someone sit with — without dismissing what was real, and without endorsing whatever the experience seemed to claim.
A Deeper Continuity
What I find most valuable about Letheby's framework is that it connects psychedelic experience to a broader question that applies far beyond psychedelics.
This same question shows up in religious experience. Mystical states in meditation. Encounters with grief, beauty, or terror that feel revelatory. Moments when ordinary reality seems to peel back and reveal something underneath. People throughout history have had experiences that produced powerful conviction about the nature of things — and the question of how to hold those convictions has been a perennial one for human beings.
The traditional contemplative answer, in many wisdom traditions, has been go slowly. Hold the experience without rushing to conclusions. Let it work on you. See what remains after months and years. The teacher's job, in many traditions, is partly to keep the student from getting attached to particular experiences or convictions — to keep the inquiry open rather than closing it down with premature certainty.
Letheby is, in a sense, applying this same wisdom to the modern question of psychedelic experience. The experiences are real. They may produce genuine insight, particularly into the constructed nature of the self. They also produce conviction that can outpace evidence, and the careful work is holding both — the depth and the humility — at once.
A Closing Thought
What's available in a careful psychedelic experience, on Letheby's view, isn't access to ultimate reality. It's something more modest and more useful: a direct, embodied recognition that you are not what you thought you were. That the self you've been suffering inside is one of many configurations your mind could take. That the patterns you've assumed were essential to who you are are, in fact, optional.
This is real knowledge. It's not the same as metaphysical certainty about the universe, but it doesn't need to be. It's enough to support meaningful psychological change. It's enough to open doors that ordinary consciousness keeps closed. It's enough, often, to make people's lives meaningfully better.
What it asks in return is a kind of intellectual humility. The willingness to hold what you've experienced without immediately codifying it. The capacity to let an experience continue to work on you without rushing to install conclusions. The patience to let depth become wisdom over time rather than mistaking the felt force of an experience for the truth of every claim that emerges from it.
This may be the most important integration skill there is. And it applies whether you've ever taken a psychedelic substance or not.
If you'd like to explore what careful, clinically informed integration of psychedelic experiences could look like — or to think through how to hold profound experiences of any kind without losing yourself in them — you're welcome to book a consultation.
Psychedelics: From Breakthrough to Backlash—and Back Again
The story of psychedelic medicine is often told as a heroic return after fifty years of unjust suppression — but the honest history includes both real promise and real problems, including the 2024 FDA rejection of MDMA-assisted therapy after serious ethical violations surfaced. A therapist on the full history, the current reckoning, and what responsible psychedelic care actually requires.
The story of psychedelic medicine is often told as a heroic one.
In the telling, scientists in the 1950s discovered remarkable therapeutic potential in compounds like LSD, MDMA, and psilocybin. They published hundreds of papers, treated thousands of patients, and were on the verge of transforming psychiatry. Then came the 1960s — countercultural excess, public backlash, and finally the 1970 Controlled Substances Act, which classified most psychedelics as Schedule I and effectively ended the research.
For fifty years, the story goes, this powerful family of medicines sat unused while millions suffered with conditions they might have helped. Now, thanks to a small group of dedicated researchers and a new generation of clinical trials, psychedelics are finally returning to medicine — and not a moment too soon, given the depth of the contemporary mental health crisis.
This narrative is largely true. It's also incomplete. And the parts it leaves out matter.
I want to walk through the actual history of psychedelic medicine — the early promise, the legitimate concerns, the long suppression, the renaissance, and the very real reckoning the field is currently going through. Because the work Path of the Pearl is positioned around — bringing psychedelic-assisted therapy carefully into legitimate clinical practice — depends on being honest about both what these medicines can offer and what's gone wrong, even recently, when they've been used without sufficient care.
The Forgotten Era of Scientific Optimism
The history before the 1970 shutdown is genuinely remarkable.
After Albert Hofmann's accidental discovery of LSD's psychoactive effects in 1943, psychedelics quickly became serious research tools. Through the 1950s and into the 1960s, mainstream universities, hospitals, and pharmaceutical companies investigated their potential. Studies were funded by reputable institutions. Findings were published in respected journals. By some estimates, more than 1,000 papers were published and tens of thousands of patients received psychedelic-assisted treatment during this era.
The early findings were striking, especially for conditions that had been resistant to other treatments. Alcoholism. Severe depression. Anxiety. Trauma. End-of-life distress. Some of the research foreshadowed exactly what later studies have rediscovered: that under the right conditions, psychedelic experiences could produce lasting psychological changes that ordinary treatment had not achieved.
It would be wrong to romanticize this era. The standards of clinical research were less rigorous than they are today. Many studies lacked proper controls. Informed consent was not what it is now. The line between researcher and patient was sometimes blurred. Some of what was called therapy would not pass ethical review today.
But the scientific interest was genuine, and the early signal was real. The compounds were doing something that seemed to matter.
What Actually Went Wrong
The collapse of psychedelic research wasn't driven entirely by politics, though politics was a major factor. The fuller story involves several converging problems.
Excesses outside the lab. Psychedelic use expanded rapidly beyond clinical and research settings in the 1960s. Recreational use grew. Some users had genuinely harmful experiences. Cases of prolonged psychosis, suicide, and psychiatric hospitalization made the news. The medicines that had been used carefully in supervised settings began to be used carelessly in entirely different ones, and the predictable harms followed.
Loss of institutional control. Figures like Timothy Leary moved beyond research and into advocacy, encouraging widespread use. Whatever Leary's other merits, his approach undermined the scientific case. The medicines came to be associated with countercultural rebellion rather than with rigorous medicine.
Genuine policy concerns. Some of the regulatory caution wasn't only political. The early research period had produced cases of harm that hadn't been adequately addressed. The infrastructure for safe administration outside clinical settings didn't exist. Even responsible researchers had concerns about how widely use was spreading and what the consequences might be.
Political opportunism. The Nixon administration's response was clearly political, and the 1970 Controlled Substances Act placed all classical psychedelics in Schedule I — the most restrictive category, with no recognized medical use and severe limitations on research. This designation was disproportionate to the evidence and, in retrospect, has been widely criticized. But it didn't emerge from nothing. It emerged from a combination of real concerns and political calculation.
The consequence was decades of effective research silence. Studies didn't completely stop, but the regulatory and funding barriers made them extraordinarily difficult. Most academic researchers moved to other topics. The compounds remained in clinical memory primarily as something to be cautious about, and the careful clinical work of the previous era was largely lost.
The Cost of the Silence
It's worth pausing on what this silence cost.
For fifty years, while psychedelics sat unused, mental health conditions worsened in many populations. PTSD became increasingly recognized but remained difficult to treat. Treatment-resistant depression affected millions, with limited options after standard medications failed. Addiction continued to devastate communities. Suicide rates rose. Overdose deaths reached crisis levels. Anxiety and depression became, by some measures, the defining mental health challenges of the era.
Meanwhile, pharmaceutical innovation in psychiatry slowed dramatically. The major pharmaceutical companies, frustrated by the high failure rate of psychiatric drug development, scaled back their psychiatric programs. The treatments available in 2020 looked largely similar to the treatments available in 1990, and the people they didn't help remained without options.
Whether or not psychedelics would have closed this gap is impossible to know. The early research, while promising, was not rigorous enough to justify confident claims. But the absence of serious investigation during fifty years of growing mental health crisis represents, at minimum, a missed opportunity to find out.
This is part of what drove the renewed interest beginning in the late 1990s and accelerating through the 2010s. A new generation of researchers, often working at academic institutions like Johns Hopkins, NYU, and Imperial College London, began carefully picking up the work that had been abandoned. The early results were striking. Studies on psilocybin for treatment-resistant depression, end-of-life anxiety, and addiction produced effect sizes that conventional treatments rarely matched.
The psychedelic renaissance was underway.
The Renaissance and Its Cracks
For most of the 2010s, the story was straightforwardly hopeful.
Clinical trials were producing impressive results. The FDA granted Breakthrough Therapy designation to MDMA-assisted therapy for PTSD in 2017 and to psilocybin for depression in 2018. Major academic centers established psychedelic research programs. Investment poured in. Oregon and Colorado moved forward with state-level legalization of psilocybin therapy. The field appeared to be on a steady trajectory toward FDA approval and mainstream integration.
Then, in August 2024, the FDA rejected MDMA-assisted therapy for PTSD.
The rejection was a shock to many in the field. The clinical trials, on their face, had shown impressive results. The need for new PTSD treatments was unquestionable. The expectation, both inside and outside the field, was approval.
The reasons for rejection were sobering. They tell a story the field is still grappling with, and one that anyone considering psychedelic-assisted therapy deserves to know.
Functional unblinding. MDMA produces effects so distinctive that participants and therapists could almost always tell whether they had received the drug or a placebo. This undermines the basic logic of the placebo-controlled trial. The FDA noted that expectancy effects became indistinguishable from pharmacological effects.
Selection bias. Many participants in the trials had used MDMA before and entered expecting benefit. This is a population unlikely to produce regulatory-grade efficacy data.
Standardization problems. The psychotherapy component of the treatment wasn't standardized in a way that would allow it to be reliably reproduced. The MAPS treatment manual incorporated elements from over a dozen different psychotherapeutic approaches, and the FDA noted that this lack of standardization made it difficult to know what would actually be approved.
Adverse events. FDA inspections uncovered unreported adverse events at multiple sites. The agency's review concluded that Lykos had not adequately characterized the drug's safety, acute effects, duration of impairment, or abuse potential.
Ethical violations. Most seriously, allegations of therapist sexual misconduct at a Phase 2 trial site in Canada led to retraction of three peer-reviewed papers in August 2024. The therapist involved was accused of sexually assaulting a research participant during her MDMA experience. The ICER review concluded that sexual boundaries were severely crossed with at least one patient in a Phase II trial. The participant's case has been the subject of extensive reporting and a podcast investigation.
These are not minor concerns. The patient who was harmed had come into the trial seeking help for PTSD. She left having been sexually assaulted by her therapists while in an altered state. The institutional response from MAPS — the organization that conducted the trial — has been the subject of significant criticism, including allegations of inadequate transparency and a culture that allowed boundary violations to go unaddressed.
The Lykos/MAPS situation isn't the entire field. But it points to real problems that the broader psychedelic medicine movement has had to reckon with.
What This Has Taught the Field
The MDMA rejection forced an honest reckoning.
The lessons being absorbed by researchers and clinicians include:
Boundary violations during altered states are uniquely dangerous. Patients under psychedelics are particularly vulnerable. Their judgment is altered, their defenses are softened, their capacity to refuse or report is compromised. Therapist sexual contact is always a serious violation; with patients in psychedelic states it is profoundly so. The field has begun to develop stricter standards, more rigorous training requirements, and better oversight structures — though much work remains.
The therapy component needs to be standardized. If a treatment is going to involve both medicine and psychotherapy, the psychotherapy has to be defined clearly enough that what's being tested can be reliably reproduced. Treatments built around proprietary, multi-approach, hard-to-replicate therapeutic frameworks pose real regulatory and ethical problems.
Adverse events must be reported. Underreporting of difficult experiences and adverse outcomes — out of misplaced enthusiasm for the field, or self-interested protection of the research, or simple inadequate procedures — has been a real problem. The field is now building better infrastructure for honest adverse event reporting.
Functional unblinding is a structural problem. When a drug's effects are obviously different from a placebo, the placebo-controlled trial model breaks down. The field is exploring alternative trial designs, including active placebos and dose-finding approaches, but no full solution has emerged.
Advocacy and science don't mix well. MAPS was both a research organization and an advocacy organization with deep emotional investment in MDMA's approval. The conflict between these roles appears, in retrospect, to have compromised the integrity of the research in ways that were difficult to see from inside the organization.
These lessons matter because the next significant test is approaching. Compass Pathways completed two positive Phase 3 trials of psilocybin for treatment-resistant depression — COMP005 in June 2025 and COMP006 in February 2026. The company is targeting a New Drug Application submission in Q4 2026, with a potential FDA decision in late 2026 or early 2027. Whether psilocybin receives approval — and whether other psychedelic therapies follow — will depend in significant part on whether the field has actually learned what the MDMA rejection was trying to teach it.
What This Means for Where We Are
The honest picture of where psychedelic medicine stands right now is complicated.
The clinical promise remains real. Studies continue to show that psychedelic-assisted therapy can produce changes in conditions like treatment-resistant depression, end-of-life anxiety, and certain addictions that other treatments have not reached. The neuroscience has advanced significantly, and there are now coherent biological models of why these compounds work the way they do.
At the same time, the field is in a real moment of reckoning. The MDMA rejection was not simply a regulatory setback. It surfaced genuine problems — about ethics, about study design, about institutional culture, about how to integrate medicine and psychotherapy responsibly. Some of these problems were always present. Some have grown as the field has expanded into territory it wasn't quite ready for.
State-level legalization adds another layer of complexity. Oregon's Measure 109 and Colorado's Proposition 122 have opened legal psilocybin therapy in those states ahead of federal approval. These programs have produced both genuine help for patients and real concerns about quality control, training standards, and oversight. The infrastructure for safe psilocybin therapy outside the federal regulatory framework is still being built.
Outside the clinic and state programs, an underground ecosystem of retreats, ceremonies, and underground guides continues to operate. Some of this work is careful and helpful. Some is reckless. Some has caused serious harm. The current legal limbo doesn't make this work disappear; it just makes it harder to regulate.
For anyone considering psychedelic-assisted therapy, this means the choice is more complicated than it sometimes appears. Legal access is limited. The quality of available care varies enormously. The field is still figuring itself out. And the marketing — whether from retreat centers, ketamine clinics, or some psychedelic therapists — sometimes overstates what's known.
What Path of the Pearl Stands For
I want to be honest about where this practice sits in this larger picture.
I support careful, responsible development of psychedelic-assisted therapy. I believe the early clinical research and the deeper neuroscience point toward something real. I'm watching the Compass Pathways pipeline with cautious hope, and I'm preparing for what legal psilocybin therapy will require if and when it becomes available in California.
I also believe the field has serious work to do. The MDMA rejection was not unjust. The ethical violations that surfaced are not isolated incidents that can be dismissed. The standards for therapist training, boundary management, informed consent, adverse event reporting, and research integrity need to be substantially higher than they have been. Patients deserve protection precisely because the medicines are powerful and the states they produce are uniquely vulnerable.
What I try to offer at this practice is what I think the field most needs: serious depth-oriented psychotherapy as the foundation, with careful clinical use of the legal psychedelic medicines (currently ketamine) as one tool among many, with rigorous attention to preparation and integration, and with honesty about both the potential and the limits. When psilocybin therapy becomes legally available, I plan to continue this work with the same approach.
What I don't want to be is a participant in the next wave of psychedelic enthusiasm that gets out ahead of what we actually know how to do well. The history we just walked through is a cautionary tale. The field that gets this right will be slower, more careful, and more honest than the one that's been moving most loudly through the last decade.
A Closing Thought
The story of psychedelics is not a simple morality tale of suppression and return. It's a more complicated story about powerful compounds, human institutions, the difficulty of doing good research on subjective experience, and the ways enthusiasm and caution have both, at different times, failed to serve patients.
What's clear is that something real is being studied — that under the right conditions, with the right preparation, in the right relationship, with proper integration, these medicines can help people whose suffering has not yielded to other treatments. What's also clear is that the right conditions is harder to achieve than the field has sometimes acknowledged, and that getting it wrong has real costs to real people.
For anyone considering psychedelic-assisted therapy now or in the future, the most important questions aren't about whether the medicines work. They work, for some people, in some conditions, under the right circumstances. The important questions are about the circumstances. Who is providing the care. What their training and supervision look like. How they handle preparation, the experience itself, and integration. How they think about boundaries, ethics, and harm. Whether they're honest about what they don't know.
The history of this field offers both promise and warning. Both deserve to be heard.
If you'd like to discuss what careful, responsible work in this space could look like for you, you're welcome to book a consultation.
When Two Nervous Systems Meet: The Science of Co-Regulation in Healing
When two people are in close attuned interaction, their nervous systems begin to coordinate at the neural level — and recent psychotherapy research shows that this inter-brain synchrony actually increases over the course of effective treatment and correlates with symptom reduction. A therapist on what the science of co-regulation reveals about how healing happens, why the therapeutic relationship may be one of the most powerful clinical mechanisms we have, and what this means for psychedelic-assisted work.
There's a moment, in good therapy, that's hard to describe but unmistakable when it happens.
The room quiets. The client, who came in activated — heart racing, mind looping, body braced — begins to soften. Their breathing deepens. Their shoulders lower a fraction. Their voice slows. Nothing has been said that would explain the shift. The therapist hasn't offered a clever interpretation or a particularly skillful intervention. Something else has happened.
What's happened, increasingly, can be measured.
A growing body of neuroscience research — using a technique called hyperscanning, which records the brain activity of two people simultaneously — is showing something remarkable. When two people are in close attuned interaction, their nervous systems begin to coordinate. Brain rhythms align. Heart rates can synchronize. Breath patterns drift toward one another. The two separate biological systems, while remaining distinct, begin to function as a coupled system — what some researchers are now calling inter-brain synchrony.
This isn't woo. The studies are using EEG, fMRI, and functional near-infrared spectroscopy (fNIRS) — established methods of measuring brain activity. The synchrony is real, measurable, and increasingly understood to be one of the most important biological mechanisms underlying human connection.
And in 2025, researchers reported something striking: in psychotherapy, the inter-brain synchrony between patient and therapist increases over the course of treatment, and that increase correlates with symptom reduction.
I want to walk through what this means, because it changes how we understand what therapy actually does — and it illuminates something important about why relationship is at the heart of healing, in psychedelic work and in everything else.
What Co-Regulation Actually Is
You experienced this before you had language for it.
Infants don't regulate themselves. Their nervous systems are far too immature. The capacity to settle from distress, to find calm after activation, to digest food, to sleep, to feel safe — none of this is something infants do alone. They borrow it from the regulated nervous systems of the adults around them.
When a baby is upset and a caregiver picks them up, holds them close, breathes slowly, hums quietly, speaks gently — what's actually happening is that the caregiver's nervous system is doing the regulatory work that the baby's system can't yet do for itself. The baby's heart rate slows toward the caregiver's. The baby's breathing matches the caregiver's rhythm. The baby's stress chemistry quiets as the caregiver's calm chemistry transmits, through touch and sound and presence, into the baby's system.
This process, called co-regulation, was foundational to your developing nervous system. Every time you were soothed as a child, you weren't just being comforted in some psychological sense. Your physiology was being literally regulated by another body. Over thousands of these interactions, your nervous system slowly built the capacity to do some of this work on its own — what eventually becomes self-regulation in adulthood.
But here's what's important to understand: co-regulation never stops mattering. It doesn't get replaced by self-regulation. Adults regulate each other constantly. A partner's calm presence at the end of a hard day. A friend's steady listening when you're falling apart. A therapist's grounded presence when you're working with difficult material. The presence of a beloved animal. The steady voice of a parent on the phone. All of these are doing the same biological work that the caregiver did for the infant — your nervous system finding its way back to baseline by borrowing regulation from another nervous system.
This isn't poetic. It's literal. And the research is now showing us how it works at the neural level.
What the Hyperscanning Studies Are Revealing
When two people interact, their brains don't operate independently. Recent research is mapping how closely they actually coordinate.
A 2025 systematic review of 30 hyperscanning studies found that inter-brain synchrony is consistently altered in psychiatric conditions. People with anxiety, depression, borderline personality disorder, autism, and other conditions show measurable differences in how their nervous systems sync with others. Reduced synchrony, in many of these conditions, correlates with the social and interpersonal difficulties that are part of the disorder.
This is profound when you think about it. The struggles with connection that so often characterize psychological suffering aren't just psychological. They're showing up at the level of inter-brain coordination itself. The disconnection people feel isn't only in their experience — it's in their physiology.
Other research has shown:
A 2023 study by Ellingsen and colleagues found that during clinical interactions involving pain, clinicians' DLPFC activity dynamically synchronized with patients' somatosensory cortex responses — and the strength of this neural synchrony predicted the patients' perceived quality of the therapeutic alliance. In other words: how much the clinician's brain was actually attuned to the patient predicted whether the patient felt they had a real therapeutic relationship.
Studies on breath have found that when two people focus on their breathing together, EEG synchrony increases significantly across multiple brain regions. The simple act of shared interoceptive attention — feeling your own breath in the presence of another person feeling theirs — strengthens the neural coupling between you.
Inter-brain synchrony has been observed in cooperative tasks, conversation, parent-child interaction, music-making, group meditation, and everyday close relationships. The more attuned and coordinated the interaction, the more the brains involved appear to align.
This is, I think, the empirical confirmation of something therapists, parents, and lovers have always known intuitively: that something real happens between people when they're truly together. The hyperscanning research is now showing us what that something is at the neural level.
What This Means for Therapy
The 2025 study on psychotherapy and inter-brain synchrony is one of the more remarkable findings to come out of clinical neuroscience in recent years.
Researchers measured brain activity in therapists and clients during therapy sessions across multiple weeks of treatment. What they found was that inter-brain synchrony between patient and therapist increased over the course of therapy. And that increase wasn't incidental — it correlated with measurable symptom reduction. The more the brains coupled, the more the patient improved.
This challenges a particular assumption about what therapy is doing. The dominant cultural model treats therapy as primarily about content — the insights, the techniques, the cognitive reframing, the processing of memories. The relationship between client and therapist is often framed as a context in which the real work happens.
The research is increasingly suggesting that the relationship itself may be one of the most important mechanisms — not the context for the work, but a substantial part of the work itself. The slow, gradual coupling of two nervous systems over time, in steady weekly sessions, may be doing as much therapeutic work as anything explicit being said.
This makes sense in light of how human nervous systems develop. They learned to regulate through relationship. They continue to need relationship to update. When old patterns are stuck — particularly the patterns laid down in early caregiving relationships — they often can't be reached through cognitive work alone. They were laid down in the body, in interaction with another body. They tend to need to be reached the same way.
A therapist's calm, attuned, dependable presence — week after week, year after year — is not just supportive. It's doing direct neurobiological work on the patient's nervous system. The patient borrows regulation, repeatedly, until something starts to update. The brain that had been organized around chronic dysregulation begins to organize around something else.
This is, in many ways, what depth therapy has always understood but lacked language for. The Freudians called it transference. The relational analysts called it the therapeutic alliance. Stephen Porges, with his polyvagal theory, has reframed it as the activation of the social engagement system through co-regulation. Allan Schore and Bonnie Badenoch have written about right-brain-to-right-brain attunement as the primary healing process. The hyperscanning research is now showing, with neural data, what these clinicians have been describing for decades.
Why This Matters for Psychedelic Therapy
This research has particular implications for the kind of work Path of the Pearl is oriented toward.
In conventional psychotherapy, the relationship matters but the medicine isn't part of the picture. In psychedelic-assisted therapy, the medicine is doing significant work — but the relationship between client and therapist arguably matters more, not less.
Here's why. During psychedelic experiences, the nervous system is in a particularly open and vulnerable state. The usual defenses are softened. Material that ordinarily stays guarded can surface. The client is, in some sense, more available to receive what's around them than they normally would be.
This means that whoever is in the room with them — whoever's nervous system is in proximity, whoever's tone and presence and breath rhythm is filling the space — has unusual influence on what happens. A therapist who is themselves regulated, attuned, present, and skilled can co-regulate the client through experiences that might otherwise be overwhelming. A therapist who is anxious, distracted, or poorly trained can fail to provide the regulation the client needs, sometimes with lasting consequences.
This is part of why the field has emphasized so consistently that the medicine alone is not the treatment. The medicine and the relationship together are the treatment. And what the relationship provides isn't only insight or interpretation. It's nervous-system support during a vulnerable state — co-regulation in the moments when the client most needs another nervous system to borrow from.
The MAPS protocols for MDMA-assisted therapy and the Compass Pathways protocols for psilocybin therapy both emphasize this. So do thoughtful Indigenous traditions and contemporary integration practitioners. The healer's role isn't only technical. It's biological. They are part of the medicine.
What This Means for Healing More Broadly
If co-regulation through relationship is one of the primary mechanisms of psychological healing, it changes how we should think about a great deal.
It means that isolation is itself injurious. Not just emotionally — biologically. People who lack consistent attuned relationships in their lives are not just lonely; their nervous systems are missing a kind of regulation that they evolved to require. Chronic loneliness has measurable effects on cardiovascular health, immune function, cognition, and mental health — and the research keeps suggesting that the mechanism involves missed co-regulation.
It means that community matters in a particular way. Not just for connection's sake, but as a source of nervous-system support that supplements what any individual can do alone. Cultures that prioritize extended family, communal living, and regular shared rhythms (meals, ceremonies, gatherings) build co-regulation into the structure of daily life. Cultures that prioritize individual autonomy often build it out.
It means that therapy is more powerful than we usually credit, and also more demanding. The presence and attunement of the therapist isn't just useful — it's doing direct biological work. Good therapy requires therapists whose own nervous systems are sufficiently regulated to do this work without depleting themselves. This is one of the reasons therapists need their own support — supervision, personal therapy, sustainable caseloads, time off.
It means that animals heal us. Research has confirmed what dog owners and equine therapists have known for years: being in the presence of a regulated mammal, particularly through touch, can substantially regulate human nervous systems. The mechanism is the same — co-regulation between two nervous systems, with the human's stress patterns gradually entraining toward the animal's calm.
And it means that what we offer each other matters more than we often realize. The friend who sits quietly with you while you cry. The partner who breathes slowly when you're spiraling. The colleague who stays grounded while everyone else panics. These aren't just nice gestures. They are nervous-system support — co-regulation in action. We are constantly regulating each other, or failing to, whether we're aware of it or not.
A Practical Note on What This Looks Like
If co-regulation is real and measurable, what helps us actually access it?
A few things the research and clinical experience point toward:
Slow breath, especially shared breath. Breathing slowly in the presence of another person whose breathing is also slow — through meditation, intentional practice, or just sitting together quietly — engages co-regulation. The research on breath-focused hyperscanning showed that even brief shared interoceptive attention strengthens inter-brain coupling.
Eye contact, when it's safe. Sustained, attuned eye contact (not staring, not analyzing) engages social engagement circuits powerfully. For many people, particularly those with trauma histories, this needs to be approached carefully — eye contact can also activate threat systems if the original experience of being looked at was unsafe. But when it works, it's deeply regulating.
Voice tone. The voice is one of the strongest co-regulatory channels we have. A warm, low, slow voice activates the parasympathetic nervous system. Polyvagal theory specifically identifies the voice as one of the primary tools of social co-regulation. Therapists, parents, and lovers know this implicitly — but it's worth being conscious of how you use your voice with people you care about.
Touch, when it's wanted and consensual. Physical contact between safe people is one of the most powerful regulatory mechanisms available. Holding hands. A hand on the shoulder. A hug. The presence of a hand on the back during difficulty. The research on touch and co-regulation is remarkable — even brief, light touch can produce measurable changes in stress chemistry within minutes.
Steady, embodied presence. Sometimes the most regulating thing a person can do for another is simply be in the room, settled, breathing, available. Not problem-solving. Not advising. Not even talking much. The presence itself is medicine.
These aren't techniques in the manipulative sense. They're ways of inviting your own nervous system into a state that can offer co-regulation to another. They work best when they emerge naturally from genuine care, not from script.
A Closing Reflection
What I find most moving about this body of research is what it confirms about something so often dismissed.
For much of modern psychological thinking, the inner life has been treated as primarily individual — your mind, your suffering, your healing. Other people show up as factors in your environment, but not really as part of who you are.
The co-regulation research is challenging this picture. It suggests that we are not the separate, self-contained selves we've been taught to be. We are nervous systems shaped by other nervous systems, regulating against and through each other, more interdependent than the cultural story has acknowledged.
This is sometimes framed as a loss of independence. I think it's the opposite. It means that healing is available in ways we hadn't fully understood. It means that the people in your life — the steady presences, the attuned therapist, the calm friend, the regulated animal, even the rare encounter with a stranger whose presence somehow settles you — are not just nice to have. They are part of how you continue to become well.
And it means that you, in turn, are part of how others become well. The presence you bring into the rooms you enter is doing work, whether you know it or not. The regulated nervous system is medicine for everyone around it. The dysregulated one transmits, too.
For people sitting with chronic patterns of suffering, this is hopeful information. You are not alone with your nervous system, even though it can feel that way. There are pathways through other nervous systems back toward the regulation your system has been seeking. Some of those pathways are professional. Some are personal. Some are communal. Some, increasingly, can involve careful work with psychedelic medicines held by skilled practitioners. But they all share the underlying mechanism: two nervous systems meeting, attuning, and slowly teaching each other something neither could learn alone.
If you'd like a place to explore what this kind of relational work could look like for you, you're welcome to book a consultation.
From Ego to Eco: How Psychedelics Change Our Sense of Connection
Psychedelic research has found something surprising: people who experience ego dissolution during psychedelic experiences emerge with lasting, measurable increases in how connected they feel to the natural world — sometimes for years afterward. A therapist on what this finding means for psychological healing, for eco-anxiety, and for the modern condition of disconnection.
One of the most consistent findings in psychedelic research is also one of the strangest, and the one I think gets the least attention in popular conversation.
People who have profound psychedelic experiences often emerge with a lasting, measurable change in how connected they feel to the natural world.
Not as a metaphor. Not as a fleeting mystical impression that fades within days. As a stable shift, measurable on psychological scales, persisting in some cases for two years or longer after the experience.
A growing body of research — much of it led by Robin Carhart-Harris and colleagues — has been documenting this phenomenon. The original landmark study by Hannes Kettner and his team, From Egoism to Ecoism, found that people who took psychedelic substances showed significant increases in nature relatedness — a well-validated psychological measure of how connected someone feels to the natural world — at two weeks post-experience. Follow-up research has now extended these findings, with some studies showing the changes persist for up to two years.
What predicts this shift? Two things, primarily. The depth of ego dissolution during the experience — the temporary loosening of the felt sense of being a separate self. And the environmental setting of the experience itself — sessions that happen in nature produce stronger and more lasting increases in nature connectedness than those that happen indoors.
This finding is more important than it first appears. It connects to questions about psychological healing, ecological crisis, and what it actually means to be a self. I want to walk through it carefully, because I think it's one of the more meaningful discoveries to come out of the psychedelic research renaissance.
What Nature Relatedness Actually Is
The concept of nature relatedness sounds like it might be soft — a self-report of whether you like trees. The actual psychological construct is more specific and more clinically meaningful.
Nature relatedness measures how much a person experiences themselves as part of the natural world rather than separate from it. It includes felt sense, identity, and lived experience. Someone with low nature relatedness might appreciate nature aesthetically but experience themselves as distinct from it — nature is over there, I am over here. Someone with high nature relatedness experiences themselves as embedded in, continuous with, and intrinsically connected to the natural world. The trees aren't just outside; they're somehow part of the same fabric the person is part of.
This isn't a personality quirk. Research has consistently shown that nature relatedness is associated with:
Lower rates of anxiety and depression. Higher self-reported well-being. Greater meaning in life. Higher levels of positive emotion. Reduced stress and improved cognitive function. Greater pro-environmental behavior. And — this is the part most directly relevant to clinical work — significantly better outcomes on a range of mental health measures.
In other words, the felt sense of being connected to nature isn't just nice. It appears to be one of the underrecognized pathways to psychological health.
This makes the finding that psychedelics can reliably increase nature relatedness — and that this increase mediates the therapeutic outcomes themselves — clinically significant. It suggests that part of what's healing about psychedelic experience isn't only the loosening of rigid patterns or the processing of difficult material. It's the restoration of a connection most people in modern life have lost.
What Ego Dissolution Has to Do With It
The mechanism the research keeps pointing to is ego dissolution.
Ego dissolution is the experience, during certain psychedelic states, of the felt sense of being a separate self becoming less solid. The boundaries between you and the world soften. The narrative of who you are quiets. The constant background processing that ordinarily produces the experience of being yourself, here, distinct from everything else temporarily releases its grip.
This experience can be unsettling, especially for people who haven't been prepared for it. But for many people, especially when held in supportive conditions, it's described as one of the most meaningful experiences of their lives. The walls that have always seemed to separate them from the world thin. What's left isn't nothing — it's a kind of expanded, more spacious sense of belonging.
What the research is showing is that this experience of dissolved selfhood doesn't just produce a passing impression. It produces a lasting recalibration of how connected the person feels to everything outside themselves. The wall, once it's been seen as a wall rather than as reality, doesn't quite go back up the same way.
For many people, this shows up most palpably as nature connectedness. They emerge from the experience and find that they notice trees differently. They feel an unfamiliar tenderness for animals. They recognize themselves as part of the living world in a way that had previously been intellectual rather than felt. The shift is often subtle but persistent.
It also shows up — and the research is increasingly clear about this — as social connectedness. People who experience ego dissolution often report lasting increases in their felt sense of connection to other people. They describe more empathy, more openness, more willingness to be moved by other people's experiences. The boundary that dissolved wasn't just between self and nature. It was between self and other, more broadly.
A 2025 review paper proposes that what psychedelics may produce is a generalized self-other overlap — a softening of the boundary that ordinarily separates the self from everything else, with implications for connection to nature, to other people, and to life as a whole.
Why This Matters in This Moment
I want to spend some time here because the finding intersects with something I see often in my practice, and that I think more therapists need to be naming.
Many of my clients are quietly suffering from forms of distress that don't have neat clinical names. A vague but persistent sense of disconnection — from themselves, from others, from the world. A grief they can't quite articulate about the state of nature, the loss of biodiversity, the climate news that arrives daily. A loneliness that goes deeper than relationships, into something more existential.
The term eco-anxiety has begun to enter clinical conversation, though it's still underdeveloped. What I see in clients includes that and goes beyond it. It's a particular kind of suffering that comes from living inside the contemporary version of human selfhood — separated from the rest of the living world, individuated to the point of isolation, identified with a self that's measured by achievement and consumption rather than belonging.
This isn't the same as depression in any standard diagnostic sense. It's something closer to what the eco-philosopher Joanna Macy has called the great unraveling — the inner correlate of an ecological crisis that's actually happening around us. People feel it. Most don't have language for it. And the cultural script tells them to keep going, keep working, keep consuming, keep producing — even as something inside them knows that the disconnection is itself a kind of wound.
What the psychedelic research is suggesting is that this disconnection isn't permanent. The felt sense of being separate from the natural world is not a fixed feature of being human. It's a construction — culturally, neurologically, developmentally — that can change.
Indigenous traditions have known this forever. Many contemplative traditions have known it. Now, the research is showing it neurologically. And for people who are quietly suffering from the modern condition of disconnection, this is a meaningful piece of information.
Why Setting Matters So Much
The Kettner study and several that have followed found something specific about where the experience takes place.
People who had psychedelic experiences in natural settings showed larger and more lasting increases in nature relatedness than those who had experiences indoors. The medicine and the environment combined — neither alone produced the same effect.
This makes sense in light of how psychedelics work. The medicine softens the predictive scaffolding that ordinarily structures experience. What replaces that scaffolding, temporarily, is whatever the person is actually encountering. If the encounter is with trees, sky, water, the texture of soil, the rhythm of wind, the surrounding life of a forest or shoreline — the new experience that consolidates in the brain has those elements woven through it.
If the encounter is with a clinical room, fluorescent lights, and a screen, the experience integrates around those.
This isn't a value judgment about clinical settings — they have important uses, particularly for people whose suffering requires the safety and structure of a controlled environment. But it's a reminder that set and setting aren't soft variables in psychedelic work. They shape what gets built during the experience and what consolidates afterward.
For traditions that have used these medicines ceremonially for thousands of years, this isn't news. Many Indigenous psychedelic traditions take place in or near specific natural settings, often connected to sacred land, with the natural world understood as part of the medicine itself. The research is now describing, in neurological language, something traditional practitioners have long known.
What This Tells Us About Healing
This research changes how I think about psychedelic-assisted therapy, and about therapeutic work more broadly.
For a long time, clinical psychology has framed mental health primarily as an internal matter. Fix the thoughts. Process the trauma. Regulate the nervous system. Build healthier internal structures.
These are real and important. But the research on nature relatedness suggests something additional: that part of what's actually wrong in many forms of psychological suffering is relational in a deeper sense than therapy ordinarily considers. Not just our relationships with other people, though those matter. Our relationship with the living world we're embedded in.
When that relationship is severed — and modern life severs it in countless small ways — people don't always know how to name what's missing. They feel disconnected, anxious, depressed, restless, but the conventional categories don't quite capture what's actually happening. They've lost something fundamental about being a living creature among other living creatures, and the loss is so culturally normalized that it goes unnamed.
What psychedelic experiences can offer, in this view, isn't only an opening into difficult inner material. They can also offer a temporary restoration of a connection that's been culturally suppressed. The experience of being part of the living world rather than separate from it. The recognition that the boundary between self and nature, while useful for some purposes, isn't fundamental.
When this connection is felt directly, something can change that no amount of cognitive understanding alone produces. People come back from these experiences and their lives often look different — not because they've solved anything in particular, but because they've remembered something about being alive that they had forgotten.
How This Can Show Up Without a Medicine
I want to be careful not to suggest that psychedelics are the only path to this kind of shift. They aren't. The research keeps pointing back to the underlying mechanism — self-expansion, self-other overlap, the softening of the boundary between self and world — which can happen through many pathways.
Time in nature, especially time spent slowly and attentively, increases nature relatedness even without any medicine. Studies have shown this consistently. A daily walk in a natural setting, with attention turned outward, gradually shifts the felt sense of self over weeks and months. Not dramatically, but real.
Contemplative practice produces similar shifts. Sustained meditation, particularly the practices oriented toward non-dual awareness, also softens the boundary between self and world. People who've practiced for years sometimes describe a similar quality of belonging that psychedelic experiences can produce more rapidly.
Deep relational experiences can do this — extended time with another being whose presence quiets the usual narrative of separation. People often describe this in the company of certain animals, with elders or wise teachers, in caregiving relationships, in long-term romantic partnerships that have moved beyond the early relational dynamics into something more spacious.
Even ordinary moments can produce small versions of this shift. Sunset light. The texture of moss. A child sleeping. The sound of wind in trees. Many of us have felt, in such moments, a brief loosening of the sense of being a separate self — a quiet recognition that we belong to something larger.
The psychedelic experience can produce these states more reliably and more powerfully. But the shift it produces isn't qualitatively different from what's available, in subtler forms, in ordinary life. The medicines may amplify and accelerate a recognition that's always available to anyone willing to attend carefully.
A Closing Reflection
What I find most meaningful about this research isn't the clinical implications, though those matter. It's the philosophical implication.
The deep assumption of modern Western life — that we are separate selves, individuated and self-contained, distinct from the natural world and from each other — turns out to be one possible configuration of consciousness, not the only one. There are other ways to experience being alive. The walls can soften. The connection can be felt directly.
For people in psychological distress, particularly the modern forms of distress that involve disconnection, isolation, and the felt absence of meaning, this is hopeful information. Whatever sense of separation has been organizing your suffering is not the final truth about who you are. It is one model your brain has been running. The model can soften.
For the larger questions of our moment — ecological grief, climate distress, the felt unraveling of the natural world we're all part of — this research offers something else. The disconnection many of us have been living inside is not just our individual problem. It's a cultural condition, and it has individual consequences. But the connection that's been lost is not gone. It's recoverable.
This is, I think, part of why psychedelic therapy has felt so important to so many people in this moment. Not because the medicines are magic. Not because they fix anything in particular. But because they can help people remember something that the world we've built has obscured: that we belong to the living world, that we are not alone in it, that the wall between self and nature is more provisional than it seems.
If you'd like to explore this kind of work — through depth therapy, integration support, contemplative practice, or some combination — you're welcome to book a consultation. And whether or not psychedelic experience is part of your path, the recognition this research points toward is available, in quieter forms, to anyone willing to look for it.
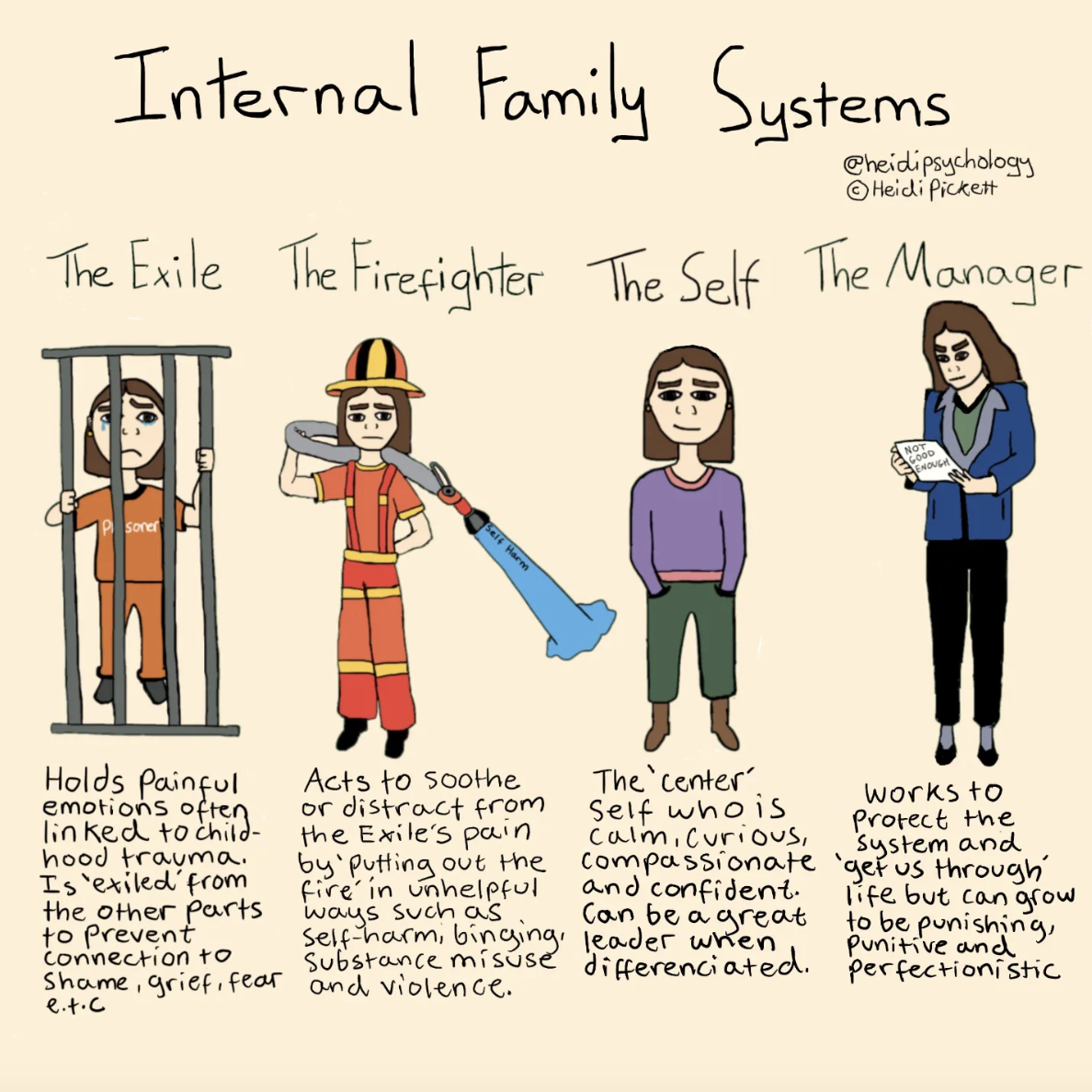
What Is Internal Family Systems — and Why It Fits Psychedelic Work So Naturally
Internal Family Systems, developed by Richard Schwartz, sees the mind as a system of distinct parts — protectors, exiles, and a core Self — and has emerged as one of the most natural frameworks for psychedelic-assisted therapy. A therapist on what IFS actually is, why Schwartz himself has called psychedelics a way to reach material that protectors won't ordinarily let near, and what an IFS-informed psychedelic session can do.
There's a model of the mind that, once you start using it, becomes hard to see things any other way.
It's called Internal Family Systems, or IFS — developed by psychologist Richard Schwartz in the early 1980s. Schwartz started as a family therapist, working with the kinds of difficult dynamics that play out between people in households. He noticed, listening carefully to his patients, that they kept describing something similar happening inside themselves. Different voices. Different reactions. Parts of them that wanted different things, that argued, that took over, that hid.
He began to ask his patients about these parts directly. What surprised him was that they could describe them in remarkable detail. Each part had a history, a role, a job it had taken on, a relationship to other parts. The internal world, he realized, looked surprisingly like the families he'd been working with — a system of distinct individuals, each with its own perspective, all trying to coexist.
Over decades, this observation became one of the most influential models in contemporary psychotherapy. In 2015, IFS was added to the National Registry of Evidence-based Programs and Practices. A 2025 scoping review in Clinical Psychologist found it a promising approach for PTSD, depression, and chronic pain. And in recent years, IFS has emerged as one of the most natural therapeutic frameworks for working with psychedelic experiences — to the point that Schwartz himself has co-authored a new clinical manual on integrating the two.
I want to walk through what IFS actually is and why this pairing has become so important — because for people considering psychedelic-assisted therapy, or sitting with their own difficult inner experience, the IFS framework offers something genuinely useful.
The Mind as a System, Not a Monolith
Most of us were raised on a particular assumption about the mind: that there's one you inside, who has thoughts and feelings and makes decisions. When that you feels conflicted or confused — wanting one thing and doing another, knowing better and behaving worse — it's usually framed as a failure of integration, willpower, or self-knowledge.
IFS proposes something different. The mind isn't a single voice with occasional conflicts. It's a system of distinct parts, each with its own perspective, history, and concerns. What feels like confusion or self-contradiction is often just multiple parts active at once, with different agendas.
You've probably noticed this without naming it. A part of you wants to go to bed early; another part stays up reading. A part of you wants to leave a job; another part is afraid of the change. A part of you knows you should call your father; another part is still angry at him. Most of the time, we treat these as opposing impulses inside a unified self. IFS treats them as distinct parts in genuine relationship with each other, each with its own legitimate concerns.
This isn't a fringe idea. Many therapeutic traditions have recognized something similar. What IFS contributes is a precise, workable model of how the system is organized.
The Three Kinds of Parts
In Schwartz's framework, the parts that make up the inner system fall into three broad categories.
Exiles. These are parts that carry pain — usually old pain, often originating in childhood. They hold the grief, fear, shame, or loneliness that the system couldn't fully process at the time. To protect the rest of the system from being overwhelmed, exiles are usually pushed out of awareness. They don't disappear; they're held away, often for decades.
Managers. These are parts that work to prevent the exiles from being triggered. They organize your life. They keep you productive, perfectionistic, controlled, alert. They run the inner critic that pushes you to do better, the overthinker that anticipates every threat, the high-functioning self who keeps everything moving. Their job is to make sure the wounded exiles stay safely contained — by managing the external world so carefully that the underlying pain never gets stirred up.
Firefighters. These are emergency responders. When the managers fail and exiled pain starts to surface, firefighters come in to extinguish the feeling fast and by any means necessary. They show up as explosive anger, substance use, dissociation, binge eating, compulsive scrolling, impulsive behavior. They're not trying to ruin your life. They're trying to stop you from feeling something that the system has decided would be unbearable.
The key insight, and what makes IFS clinically powerful: none of these parts are bad. They're all trying to help, in the only way they know how. They've taken on extreme roles because the system needed them to. The work isn't to eliminate parts — it's to understand them, hear them, and gradually allow them to take on healthier roles.
The Self at the Center
Underneath the parts, IFS proposes, there is something else: the Self.
The Self is not a part. It's the core of who you are — and according to Schwartz, it's present in everyone, including those with the most severe trauma histories. The Self has qualities that Schwartz organized into what he calls the eight Cs: curiosity, calm, clarity, compassion, confidence, courage, creativity, and connectedness.
When the Self is in the lead — when none of the protective parts are fully active — the system can rest. Parts can communicate. Old wounds can be approached with care rather than avoidance. The whole inner ecosystem becomes more flexible.
Most people, most of the time, are not in Self. They're blended with one part or another — taken over by the manager who's running everything, fused with the anxious part, identified with the inner critic. The work of IFS therapy is helping the Self take leadership, so that parts can be in relationship with the Self rather than dominating the system.
This is harder than it sounds. Many people, when they first encounter IFS, can't easily access the Self at all. The protective parts have been in charge for so long, and so completely, that the Self has become hard to reach. Part of the slow work of IFS is precisely about uncovering the Self that's always been there, beneath the layers of protection.
How IFS Therapy Actually Works
In an IFS session, the work is direct and experiential. A therapist might invite you to notice a part of you that's been activated. The part might appear as a felt sense in the body, an image, a voice, an emotion. You're invited to turn toward it with curiosity rather than judgment.
What does this part want you to know? What's it been doing for you? How long has it been here? What's it afraid would happen if it stopped?
The part, surprisingly often, has clear answers. Once it feels seen and heard, it tends to soften. It may show you what it's been protecting — usually a younger, more vulnerable part holding old pain. The work then moves to that deeper layer: meeting the exile, witnessing what it's been holding, allowing it to be released from the burden it took on.
This is called unburdening. When an exile is unburdened, the system reorganizes around it. The managers and firefighters that have been working so hard to contain it can relax. The whole inner family becomes more peaceful.
This sounds abstract. In practice, it's deeply moving and often quite immediate. People who have done years of cognitive therapy without reaching a particular pattern can sometimes meet it directly through IFS in a single session — not because the pattern was simple, but because IFS reaches it through a different door.
Why Psychedelics and IFS Fit Together So Well
Here's where the conversation gets clinically important.
Schwartz himself, in an interview with Psychedelics Today, described what he had observed when colleagues began bringing IFS into psychedelic-assisted therapy: "There are times where you just can't convince these protective parts to let us get to an exile and heal it. And a psychedelic session can expedite that pretty easily, it seems."
This is a striking observation from one of the most influential therapists of his generation. What he's describing is a specific clinical challenge in IFS work — the protective parts that won't budge, that won't let the Self approach what they're guarding. For some people, these protectors have been in place for so long, with such conviction, that ordinary therapy can't move them. The exiles stay walled off. The healing stalls.
Psychedelics, in current neuroscientific models, work in part by temporarily softening the brain's defensive structures. Walls that have been firm become permeable. Material that's been carefully kept at a distance can come into view. From an IFS perspective, this means that during a psychedelic experience, protective parts often relax — sometimes dramatically — allowing direct contact with what they've been protecting.
What this looks like clinically: people in psychedelic states often report experiencing parts of themselves with unusual clarity. Different aspects of their psyche appear as distinct voices or images. The inner critic becomes visible as a separate figure rather than feeling like the truth. A frightened child part may show up palpably. The Self — with its curiosity and compassion — often becomes more accessible than usual.
Schwartz and his collaborators have argued that this convergence isn't coincidental. IFS and the psychedelic state share a deep structural compatibility:
Both emphasize multiplicity. IFS sees the mind as parts; psychedelic experiences often present those parts vividly.
Both prize curiosity and compassion. The qualities IFS calls Self-energy are remarkably similar to what people often access during psychedelic experiences.
Both work experientially rather than cognitively. Neither relies primarily on insight or analysis. Both engage what's happening in the moment, in the body, in direct experience of inner material.
Both seek unburdening rather than suppression. Both frameworks aim to help wounded material be released rather than managed.
When practitioners trained in both bring them together, what emerges is a coherent approach that honors what the medicine opens and provides a framework for working with what arises.
What an IFS-Informed Psychedelic Session Looks Like
In practice, a psychedelic session integrated with IFS often unfolds something like this:
Preparation. Before the session, the therapist and client may begin meeting parts together. The client learns to recognize protective parts when they show up, to differentiate them from the Self, to approach inner experience with curiosity. This preparation matters — it gives the client a vocabulary and a way of relating to whatever emerges during the experience.
The session itself. During the medicine experience, the client may encounter parts in heightened form. The therapist's role is largely to support, hold space, and occasionally offer gentle guidance — what's that part wanting you to know? Can you ask it what it's protecting? The Self, more accessible than usual, can lead the work in real time. Material that protectors had been guarding can be met directly. Old burdens that exiles have been holding can begin to release.
Integration. This is where IFS becomes especially valuable. After the experience, much of the work involves continuing the relationships that opened during the session. The parts that became visible. The exiles that began to release their burdens. The Self that emerged. Integration isn't passive — it's the ongoing practice of staying in relationship with the inner system, supporting parts that are still adjusting to new roles, allowing the reorganization that began in the session to consolidate over time.
Without this framework, psychedelic insights often fade. The parts that briefly relaxed return to their old roles. The exile that almost unburdened pulls back behind the walls. With it, the changes that began in the session can be supported, stabilized, and woven into ordinary life.
What This Means for the Larger Conversation
The growing recognition of IFS as a natural partner to psychedelic therapy reflects a broader shift in how we think about healing.
For most of the 20th century, dominant therapeutic frameworks were cognitive — fix the thoughts, change the behaviors, modify the beliefs. These work for some people, but they often don't reach the deeper layers where chronic patterns actually live.
IFS, alongside other depth approaches like somatic experiencing, AEDP, and contemporary psychoanalysis, represents a different orientation. Not fixing. Not eliminating. Understanding the system and helping it reorganize.
Psychedelic-assisted therapy, used carefully, can amplify what these approaches do. The medicine doesn't replace the work. It expands what's accessible to do the work on. The framework — IFS or another like it — provides the structure to make sense of what opens.
For people considering psychedelic therapy, this matters. The medicine alone, without a framework for working with what arises, can produce experiences that feel powerful but don't integrate. The framework alone, without the medicine, can produce gradual change that takes longer than some people have. Together, they can offer something that neither does well alone: an opening that becomes a reorganization.
A Closing Thought
What I find most beautiful about IFS, and about its convergence with psychedelic work, is the underlying premise: that beneath all of your protective patterns, beneath the wounded parts, beneath everything that has hurt you and everything you've done to protect yourself from being hurt, there is something undamaged. A core of curiosity, compassion, and presence that has been with you the whole time.
For people who have lived inside chronic suffering, this can be hard to believe. The Self can feel inaccessible, or even mythical. But it is, in the IFS view, always there. The work is not to create something new. It's to clear enough space for what's always been present to take leadership again.
Psychedelic experiences, when held well, can sometimes give people a direct encounter with this Self for the first time. Many describe it as the most meaningful experience of their lives — not because something new appeared, but because they recognized something true that had been obscured.
The work afterward is letting that Self take a more permanent role in the inner system. Not all at once. Not without setbacks. But steadily, with practice and support, the parts that have been protecting and exiling can be welcomed home, and the Self that was always there can begin to lead.
If you'd like to explore this kind of work — through depth therapy, IFS, or integration support for past or future psychedelic experiences — you're welcome to book a consultation.
When the Mind Stops Predicting
A 2021 neuroscience paper describes what meditation actually does to the brain — and the answer turns out to be remarkably similar to what psychedelics do, just slower and more gradual. A therapist on why meditation isn't really about relaxation but about loosening the predictive models that generate the suffering self, and what that means for the deepest kind of healing.
There's an old observation in contemplative traditions that goes something like this:
Beneath your thoughts, beneath your sense of being a separate self, beneath the constant narration of who you are and what's happening to you, there is something quieter — something that's been there the whole time, that doesn't need any of the rest to exist.
For most of Western intellectual history, this observation was treated as poetry, or metaphysics, or the language of religious traditions that didn't quite translate into modern terms.
In the last decade, that's been changing.
A growing body of neuroscience research is showing that what contemplative traditions have been pointing at for thousands of years can be described, with surprising precision, in the language of modern cognitive science. And what emerges from that research is something useful to almost anyone, whether or not they ever sit on a meditation cushion.
In particular, a 2021 paper by Ruben Laukkonen and Heleen Slagter — published in Neuroscience and Biobehavioral Reviews under the title "From many to (n)one: Meditation and the plasticity of the predictive mind" — offers one of the clearest scientific accounts I've seen of what meditation is actually doing to the brain. And it lines up, beautifully, with what people who've practiced for a long time have always said it was doing.
I want to walk through this — because the implications reach well beyond meditation itself. They illuminate something important about the work of healing, the relationship between contemplative practice and psychedelic experience, and what the deepest forms of psychological change actually require.
What Your Brain Is Always Doing
To understand what meditation undoes, it helps to start with what the brain is constantly doing in ordinary consciousness.
Recent neuroscience has converged on a picture of the brain as a prediction machine. Rather than passively receiving the world, your brain is actively generating predictions — about what you're seeing, what you're hearing, what your body is doing, what's about to happen, what kind of person you are, what other people think of you, what's going to come next.
These predictions operate at many levels and time scales:
Some are immediate and concrete — the prediction that the next sound from a familiar voice will be a familiar word, the prediction that your foot will meet the step you're about to take.
Some are more abstract — predictions about how the day will unfold, how a relationship is going to feel, how you'll perform at the meeting tomorrow.
Some are very long-term — predictions about who you are, what kind of person you've always been, what your life means, what you can and can't do.
The brain runs all of these constantly, mostly outside of conscious awareness. The smooth flow of ordinary experience is largely the felt result of these predictions matching reality well enough that you don't notice them happening. You only become aware of the prediction machinery when something goes wrong — when the step isn't where you expected, when someone responds in a way you didn't anticipate, when your sense of who you are gets challenged.
The deepest of these predictions, the ones running at the highest levels of abstraction over the longest time scales, are what produce the felt sense of being you. Your continuous identity. Your narrative self. The story of who you are.
What Meditation Actually Does
Here's where Laukkonen and Slagter's framework becomes interesting.
In their account, meditation works by progressively reducing these predictive processes — not all at once, but in a particular order, from the most abstract and long-term predictions inward toward more immediate experience.
This happens through what they describe as a continuum of meditative practice:
Focused attention — the earliest stage of practice — works by stabilizing attention on a chosen object (the breath, a mantra, a sensation). This reduces distraction and quiets the most superficial layer of prediction: the constant low-level chatter about what's next.
Open monitoring — a more advanced practice — involves observing whatever arises in awareness without grasping or rejecting. This loosens the next layer: the automatic interpretive patterns that filter raw experience through learned categories. Thoughts still arise, but their hold weakens.
Non-dual awareness — the deepest forms of practice — works directly on the most fundamental predictive layer: the distinction between observer and observed, self and world. As this loosens, the felt sense of being a separate self can soften, sometimes dissolve entirely.
At each stage, the brain is doing less predicting and more experiencing. The complex, layered architecture of self that generates ordinary consciousness becomes simpler, lighter, less insistent.
This is what the paper's title — From many to (n)one — gestures toward. The many layers of selfhood gradually fall away. What remains is not nothing. It's experience itself, without the elaborate self-model that ordinarily organizes it.
This sounds esoteric. It's actually quite concrete in lived experience. Anyone who's had a moment of being fully present — watching the light through a window without naming it, hearing music without thinking about anything else, walking in nature with no internal narration — has briefly experienced what the deeper meditative states reach more fully. The thinking-about-yourself layer quiets. What's actually here becomes more vivid. The sense of being a separate observer softens.
Insight as Subtraction, Not Addition
One of the most striking ideas in the Laukkonen and Slagter paper concerns what insight actually is.
In ordinary thinking, we assume that insight comes from adding something — new information, a new perspective, a new way of seeing the problem.
But the paper proposes something different. Real insight, in this framework, often comes from removing something. The brain's models simplify. Unnecessary assumptions drop away. The complexity that had been obscuring something falls. And what was always there becomes visible.
This is consistent with how meditators describe their deepest realizations. Not as the arrival of new content, but as the recognition of something that was always already there, briefly seen clearly when the layers of model and narrative thinned enough to allow it.
This has clinical implications I find moving. So much psychological suffering is, in a sense, the accumulation of models — beliefs about who you are, predictions about what's coming, narratives about why things happened, identities you've taken on, stories you've inherited. These accumulate over years. They start to feel like reality itself.
The work of healing, in this view, isn't always about adding healthier beliefs. Sometimes it's about gently dissolving the unhelpful ones — letting the brain's predictive machinery simplify, letting the over-elaborated self-model lighten, letting something more essential come back into view.
This is what people often report after sustained meditation practice. Not new beliefs about themselves, but a thinning of the old ones. A spacious sense that they're somehow more here and less defined.
Why This Matters Beyond Meditation
You might be reading this and thinking: I'm not going to become a serious meditator. What does this have to do with me?
Here's what I'd offer.
The framework Laukkonen and Slagter describe isn't really about only meditation. It's about the deeper principle that your sense of self, your patterns of suffering, your predictions about the world — all of these are constructions your brain is generating, and constructions can be modified.
This is hopeful in a way that the medical model often isn't. You are not a fixed thing with permanent features. The depression you've lived with isn't a permanent diagnosis written into your bones. The trauma patterns aren't a life sentence. The identity you've taken on isn't who you are; it's who your brain has been predicting you to be.
The predictions can change. The models can soften. The constructions can be revised.
This happens through many pathways. Meditation is one of the most direct. Psychotherapy is another, particularly the kinds that work at depth, with the body, in relationship. Psychedelic experiences, as we'll see below, are a third. Major life transitions, encounters with art or nature that move you, deep contemplative experiences in religious contexts — all of these can produce the kind of model-simplification that the paper describes.
The path matters less than the underlying mechanism. What's needed is some sustained experience that loosens the rigid models the suffering self has been running on, and lets something more essential reorganize.
Meditation and Psychedelics as Two Routes to the Same Place
This is where the paper opens up a beautiful insight that's directly relevant to Path of the Pearl's work.
If meditation works by gradually reducing the brain's predictive processes — softening the elaborate self-model, simplifying the layers of prediction — then it's doing, slowly, what psychedelics appear to do quickly.
Both psychedelics and deep meditation increase what neuroscientists call neural flexibility — the brain's capacity for new patterns, new configurations, new ways of organizing experience. Both can produce experiences of dissolved selfhood, expanded awareness, present-centered consciousness, and the recognition that the ordinary self is a construction rather than a fixed feature of reality.
The mechanisms appear to be related. Both reduce top-down predictive control. Both loosen the rigid scaffolding through which we ordinarily organize experience. Both create openings in which the deeper, more essential mind can be glimpsed.
What differs is the path. Psychedelics produce the opening rapidly, through pharmacology. Meditation produces it gradually, through trained attention. One is dramatic and brief; the other is patient and cumulative. Each has gifts and limitations.
What's clarifying about seeing them through the same lens is the recognition that they're not opposites. They're complementary routes to the same territory. People who do both, mindfully, often find that they reinforce each other — meditation deepens what the medicine opens; the medicine reveals what meditation has been working toward.
This is part of why so many psychedelic traditions — Indigenous, Asian, contemporary therapeutic — embed the medicine work within ongoing contemplative practice. The medicine is not the destination. It's a doorway that the practice keeps open.
What This Means for the Work
For people sitting with patterns of suffering — depression, anxiety, trauma, the chronic sense of not quite being okay — this framework offers something specific.
Your suffering is partly a problem of overly rigid models. Not just thoughts, but the deeper predictive scaffolding that generates the experience of being you. These models accumulated over years, often originated in environments where they were adaptive, and have outlived their usefulness.
The work of healing involves simplifying these models, not adding more. This is one reason why people who have done a lot of therapy sometimes find themselves more burdened, not less — they've accumulated insights, frameworks, names for their patterns, stories about their wounds, without necessarily letting any of the underlying scaffolding actually simplify.
Practices that reduce prediction help. Meditation. Somatic work that brings you out of narrative and into the body. Time in nature where conceptual thinking quiets. Art that interrupts the usual filters. Therapy that holds space for the not-knowing. All of these slowly thin the layers.
Psychedelic therapy may have a specific role. For people whose models have become particularly rigid — locked depression, calcified trauma patterns — the medicine can produce a window in which deeper restructuring becomes possible. But the work continues afterward, through the slow practice of letting the new openings consolidate.
The deepest change isn't fixing yourself. It's letting the self soften enough that something more essential can come back into view. This isn't loss of identity. It's the recovery of something that was always there, beneath the elaborate construction.
A Word About What This Isn't
I want to be careful about something, because I've seen this framework misunderstood.
The idea that the self is a construction doesn't mean the self isn't real, or doesn't matter, or should be transcended. You are not less you because your continuous identity is a high-level prediction. The construction is doing important work. It allows you to function, to plan, to be in relationships, to have a coherent life.
The point isn't to dismantle the self entirely. The point is that the self can be held more lightly. That you don't have to be defined entirely by the predictive scaffolding you've built. That there's something underneath — something more essential, more present, more alive — that can be reached when the layers thin.
For people in pain, this is liberating. The depression isn't who you are — it's a layer of prediction that has gotten stuck. The trauma response isn't you — it's a pattern your brain has been generating. The harsh inner voice isn't the truth about you — it's one of many models running in the system.
These can all change. With practice, with support, with patience, the patterns can loosen, simplify, sometimes dissolve.
A Closing Reflection
What I find most moving about Laukkonen and Slagter's framework is how it brings together two domains that have long seemed separate.
Contemplative traditions, for thousands of years, have been describing the same territory: the gradual loosening of identification with thought and self, the recovery of present-centered awareness, the sense of being more whole when one is less defined.
Modern neuroscience, recently, has begun to describe the same territory in the language of predictive processing, neural flexibility, and Bayesian inference.
Neither account is complete on its own. Together, they offer something rare: a description of the deepest forms of psychological change that honors both the wisdom of ancient traditions and the rigor of contemporary science.
What this tells me, clinically and personally, is that the work of becoming more well is also, in some sense, the work of becoming less defined. Less identified with the suffering self. Less captured by the predictive models that have been generating the pain. More present to what's actually here, beneath all the layers.
This is the work that good meditation does. It's the work that depth therapy does, when it goes deep enough. It's the work that psychedelic experiences, well held, can open. And it's a work anyone can begin, in any moment, by simply being present to what's actually arising — without needing to predict, narrate, or define it.
If you'd like a place to do this work — through depth therapy, contemplative practice, integration support, or some combination — you're welcome to book a consultation.
Why Your Brain Prefers Familiar Suffering to Unfamiliar Healing
Your brain's deepest drive isn't pleasure or meaning — it's uncertainty reduction, which means it often prefers familiar suffering to unfamiliar healing. A therapist on Karl Friston's free-energy principle, why people stay stuck in patterns they consciously want to leave, and what actually allows the underlying system to change.
There's a pattern I see often in clinical work, and it's one of the more painful ones to name.
A woman has been in a difficult marriage for fifteen years. She knows it's hurting her. She can articulate exactly what's wrong. She has the resources to leave. And year after year, she stays — not because she's weak, not because she lacks insight, not because she doesn't want change. Something deeper holds her in place.
A man recognizes that he's recreating, in every relationship, the dynamic he had with his critical father. He sees it. He can name it. And he keeps finding partners who criticize him, finds himself drawn to people who confirm what he already believes about himself, even though some part of him knows it's killing him.
A woman in recovery has been doing well for months. Then, just as life starts feeling good, an old part of her finds a reason to relapse. She's confused. She doesn't understand why she can sustain suffering more easily than ease.
These patterns aren't moral failures. They're not lack of effort. They're not even — exactly — about trauma or attachment, though those are part of the story.
There's a deeper mechanism at work, and once you understand it, a lot of stubborn human suffering starts to make sense. It comes from a body of work in cognitive neuroscience that's grown out of the research of neuroscientist Karl Friston, and the principle is called free energy minimization.
The idea sounds technical. The clinical implication is profound: your brain's most fundamental drive is to reduce uncertainty about the world — and that drive is often stronger than your drive toward well-being.
I want to walk through this, because I think it's one of the most useful frames I know for understanding why people stay stuck — and what it actually takes to get unstuck.
The Brain as Uncertainty Minimizer
In the traditional picture, the brain is motivated by familiar drives — pleasure, reward, meaning, connection, survival. These are real, and they matter.
But Friston's framework proposes that underneath all of these is a deeper motive. The brain's primary job, the principle suggests, is to reduce surprise — to minimize the gap between what it expects and what it encounters.
Not emotional surprise. Statistical surprise. The mismatch between your brain's predictions and incoming reality.
Why would this be the primary drive? Because for a living system, prediction error is dangerous. If your brain can't anticipate what's coming, it can't prepare. It can't regulate. It can't keep the organism alive. From this perspective, uncertainty itself is the most fundamental threat, and the brain has evolved a powerful, constant drive to reduce it.
You can see this drive everywhere once you start looking. You turn on lights when it's dark. You check your phone when it's been silent too long. You re-read familiar books. You return to the same restaurants. You scroll the same apps. You stay in jobs that aren't fulfilling because the unknown alternative is more uncertain than the known dissatisfaction.
Most of human behavior, on this account, isn't really about pursuing happiness. It's about reducing uncertainty about what's coming next.
This is mostly invisible to consciousness, because the uncertainty-reduction work happens beneath thought. Your brain is constantly running the calculation: what do I expect to happen, and what's actually happening, and how can I close that gap? Most of the time, you experience this as the seamless flow of ordinary life. It's only when something disrupts the predictions — a surprising event, a major change, an experience that doesn't fit your model — that the underlying machinery briefly becomes visible.
Why This Makes Familiar Suffering Stickier Than New Joy
Here's where the framework gets clinically powerful.
If your brain's deepest drive is to minimize surprise, then it has a profound preference for the familiar. Even when the familiar is painful.
The known is predictable. It generates less prediction error. The brain has built robust models of what to expect, and those models are accurate even if what they're predicting is suffering.
The unknown — including the unknown of healing — is unpredictable. The brain doesn't yet have working models for what well-being feels like, what healthy relationships look like, what life is like without the chronic pattern that's been running for decades. Even when these would be better, they generate more uncertainty.
And uncertainty, to the deep brain, registers as threat.
This explains something I see clinically that often confuses both clients and therapists: people sometimes get worse when their lives start to improve. They feel anxious when relationships become healthier. They become uncomfortable when the chronic suffering they've adapted to begins to lift. Some part of them, faithful to the principle of minimizing surprise, tries to recreate the familiar conditions.
This isn't sabotage in the moral sense. It's not weakness. It's a brain doing exactly what brains have evolved to do — preferring a predictable world, even a painful one, to an uncertain one, even a hopeful one.
What This Tells Us About Trauma
The free-energy framework illuminates something specific about trauma that other frameworks don't quite reach.
For someone who experienced trauma early in life, the brain built models of what to expect based on those original conditions. The world is dangerous. People are not safe. Closeness ends badly. Your needs won't be met. These models became deeply embedded, because in the original environment, they were accurate predictions.
Years later, the world has changed. The original threat is gone. The person is now in a context where new predictions could be more accurate — but the old models are doing their job too well. They generate predictions that match the original world. And the brain, faithful to its principle, prefers those predictions to confront new evidence that would require updating the whole framework.
This is part of why trauma survivors sometimes end up in relationships that recreate the original dynamic. Not because they want to suffer. Because the brain is doing what it always does — orienting toward the familiar, even when the familiar is harm. Reality matches the prediction. Prediction error stays low. The deep system stays calm in a way that healthier conditions wouldn't permit.
It's also why merely knowing about your trauma rarely changes the patterns. The knowing happens in the conscious mind. The prediction-making happens in deeper systems that operate by their own logic. Insight alone doesn't update the model.
Active Inference: Why You Sometimes Make the World Match Your Beliefs
Friston's framework includes a striking second insight. There are two ways to reduce prediction error:
You can update your beliefs to match what's happening.
Or you can change what's happening to match your beliefs.
Both reduce the mismatch. Both serve the principle.
This is called active inference. And it explains some of the most frustrating patterns in human relationships and life.
The person who believes she's unlovable will, often unconsciously, behave in ways that produce evidence of her unlovability. Not because she wants to. Because her brain is closing the gap between expectation and reality by changing reality. If she expects rejection, she may withdraw — and her withdrawal produces actual distance, which her brain reads as confirming evidence.
The person who believes the world is dangerous will scan for threats, interpret ambiguous situations as threatening, and avoid the experiences that might produce evidence of safety. The world remains, in his experience, exactly as dangerous as he predicted.
The person who believes she can't trust anyone will test her partners constantly, hold things back, watch for betrayal — and these behaviors often produce the very rupture she feared. Her prediction was confirmed.
This is not conscious sabotage. It's the deep system doing its job, generating evidence that confirms the model, because confirming the model reduces uncertainty.
What This Means for the Work of Change
If this framework is right, real psychological change requires something specific.
It's not enough to know a new truth. The new truth has to update the predictive models. And updating predictive models is harder than it sounds, because the brain resists predictions that contradict its existing framework. New evidence gets explained away, dismissed, or absorbed back into the old model.
What actually updates models, the research suggests:
Sustained, repeated experience that contradicts the prediction. Not a single new piece of information — a long enough exposure to new reality that the brain has to revise. The body has to feel safety repeatedly to believe safety is possible. Closeness has to be experienced over and over before the model of closeness as dangerous can soften.
Experiences powerful enough to break through the existing model. This is where psychedelic therapy may have a specific role. By temporarily loosening the predictive models, psychedelics may create windows in which new evidence can actually land — and the brain can integrate experiences that it would otherwise have absorbed back into the old framework.
Relationships that don't behave according to the prediction. A steady therapeutic relationship, a partnership that doesn't repeat the original pattern, a community that responds differently than you've come to expect. These are some of the most powerful sources of model-updating in human life, precisely because they're sustained, embodied, and hard to explain away.
Tolerating the discomfort of uncertainty. Real change usually involves a period during which the old model is loosening and the new one hasn't fully formed. This is the part that feels destabilizing, even when it's healing. The brain registers it as threat. Without support, people often retreat to the old patterns to relieve the uncertainty — even when those patterns were painful. Holding through this period, with help, is what allows the new models to actually consolidate.
The Painful Implication
There's something humbling about this framework that I want to name, because I think it's important.
If your brain's deepest drive is uncertainty reduction, then the work of healing isn't just learning new things or trying harder. It's slowly, patiently, with support, teaching your nervous system that the new is survivable. That well-being isn't a threat. That love won't necessarily disappear. That safety can be trusted. That you can let go of the old prediction without dying.
For people who grew up in chaos, who survived trauma, who lived for years inside a particular kind of suffering — this work is sometimes the hardest thing they will ever do. Not because they're weak, but because they're working against a system designed to keep the familiar familiar.
The work of becoming well, in this view, is partly a process of mourning. Mourning the predictions that have organized your life, even when those predictions caused you pain. They've been with you a long time. Their loss is real, even when their loss is liberation.
What This Means for Psychedelic Therapy
This framework also clarifies something important about why psychedelics may be uniquely helpful for certain kinds of stuck patterns.
Talk therapy, however skillful, works largely within the existing predictive models. The therapist helps you see your patterns, understand them, develop new strategies. This is valuable, but the underlying models often remain intact.
Psychedelics, in current neuroscientific models, work differently. They temporarily loosen the predictive scaffolding itself. The deep models that have been organizing your experience become briefly less confident. New evidence can land before being absorbed into the old framework. Patterns that have felt fixed can briefly be seen as patterns.
This is part of why psychedelic-assisted therapy can produce changes that other treatments have not reached — particularly for trauma, treatment-resistant depression, and other conditions involving deeply locked patterns. The medicine doesn't replace the work. It creates a window in which the work can finally reach the layer where the patterns actually live.
A Closing Thought
The free-energy principle is, in some ways, a humbling framework. It suggests that most of what we experience as choice, freedom, and intention is the surface activity of a system whose deeper job is to keep us safe through prediction. The brain we live with is older than our conscious self, and it serves a function that predates our wishes for happiness.
But it's also, I think, a hopeful framework. Because once you understand why familiar suffering is so sticky, you understand what real change actually requires. Not just insight. Not just effort. Sustained, embodied, often-supported experience of something new — repeated enough times, held carefully enough, that the deep system can finally update.
The brain that learned to expect pain can learn, eventually, to expect care. The system that built itself around survival can slowly build itself around something more. This isn't fast. It isn't simple. But it's real, and it happens.
If you're sitting with patterns that have felt impossible to shift, you're not failing. You're working against the deepest drive of the system you live in. With time, support, and sometimes the specific kind of opening that psychedelic therapy can offer, the system can be re-taught. The familiar can become something else.
If you'd like a place to begin that work, you're welcome to book a consultation.
Why Healing Lives at the Edge of Order and Chaos
Living systems — including brains — function best at the edge between order and chaos, where they're stable enough to hold form and flexible enough to change. A therapist on what this framework reveals about depression, anxiety, trauma, and why psychedelic therapy works for some people but not others.
There's a way of thinking about the mind that I find quietly transformative, and that maps onto clinical experience more accurately than most other frameworks.
It comes from the field of complex systems theory — the study of how systems with many interacting parts behave — and it applies to brains, ecosystems, weather, and the dynamics of any living thing. The central observation is this:
Living systems function best when they're balanced at the edge between order and chaos.
Too much order, and the system becomes rigid. It can't adapt. Nothing new happens. It repeats itself.
Too much chaos, and the system loses coherence. Nothing connects. Patterns can't form. Function breaks down.
But at the edge between these — at a state scientists call criticality — the system has both stability and flexibility. It can hold its form while still being responsive to new information. It can change without dissolving.
This idea has profound implications when applied to the brain. And once you see it, a lot of what happens in depression, anxiety, trauma, and psychedelic therapy starts to make sense in a new way.
I want to walk through this framework, because it's one of the most useful ways I know to understand what's actually happening — and what healing actually requires — in the kinds of suffering that don't seem to respond to simpler interventions.
What the Brain Does at Criticality
Brains, like other complex living systems, appear to naturally seek a critical state — the edge between rigidity and randomness.
In this state, neurons are doing something remarkable. They're integrated enough that activity in one region can influence others; signals can travel widely; patterns can hold together. But they're also differentiated enough that the system isn't locked into one configuration. Different patterns can emerge. New combinations are possible. Information can flow flexibly.
When the brain is in this balanced state, conscious experience is at its richest. Perception is vivid. Thought is flexible. The mind can move between focused attention and free association, between holding ideas steady and letting them recombine. We feel, in some hard-to-articulate way, alive.
When the system drifts toward too much order, experience constricts. Patterns lock. The same thoughts circle. Possibility narrows.
When it drifts toward too much chaos, experience fragments. Coherence breaks down. The thread of self and meaning gets harder to hold.
Healthy mental functioning, in this framework, isn't the absence of either — it's the dynamic capacity to live at the edge between them, with the system flexible enough to move back toward center when it drifts.
Depression as Too Much Order
This framework has been particularly useful for understanding depression.
The researcher Robin Carhart-Harris at Imperial College London — who has done some of the most influential recent work on the neuroscience of consciousness and psychedelic therapy — has proposed something he calls the entropic brain hypothesis. The central idea is that mental states can be understood along a spectrum of entropy — informational disorder, or in less technical terms, how locked-in versus how flexible the brain's activity patterns are.
On one end of this spectrum is excessive order. The brain is doing the same things in the same ways. Activity patterns are repetitive. The system has gotten stuck.
This describes, in striking detail, what depression actually feels like from the inside.
The same thoughts return. The inner narrative loops. The future looks like the past. Nothing new feels possible. Motivation, novelty, hope — all of these depend on the brain's capacity to generate fresh patterns, and in depression, that capacity has constricted.
What Carhart-Harris's work suggests is that this isn't poetic. It's literal. Depressed brains show reduced flexibility in their activity patterns, reduced complexity, reduced ability to break out of established networks. The system has drifted toward too much order.
This has clinical implications. If depression is partly a problem of excessive order, then effective treatment is partly about restoring some healthy disorder — some flexibility, some new patterns, some movement back toward criticality.
Anxiety, Psychosis, and Trauma as Too Much Chaos
The other end of the spectrum is also instructive.
When the brain's activity becomes too disordered — too much entropy, too much chaos — coherence breaks down. This can show up as:
Severe anxiety, in which the threat detection system fires across too many contexts, signals don't get appropriately weighted, and the person can't hold steady against the overwhelming variety of imagined danger.
Dissociation, in which the integration of self, body, and experience fragments under stress.
Psychotic states, in which the brain's normal capacity to maintain coherent models of self and world breaks down more profoundly.
Acute trauma activation, in which the system loses its capacity to organize experience into manageable form.
In each of these, the issue isn't too little flexibility — it's too much disorder, not enough structure. The person is, in a real sense, drowning in possibilities, intensities, and inputs that the system can't integrate.
This is part of why some people who try psychedelics have difficult experiences. If your baseline state is already drifting toward too much chaos, an experience that pushes further in that direction can be destabilizing rather than healing. This isn't a failure of the medicine — it's a mismatch between what the person needed and what the medicine offered.
Where Psychedelics Fit
This framework gives us a much more accurate picture of what psychedelics are actually doing — and why they help some people while making others worse.
Psychedelics, in Carhart-Harris's framework, increase the entropy of brain activity. They loosen rigid patterns. They move the brain toward higher disorder, more flexibility, more openness to new configurations.
For someone whose suffering is fundamentally about too much order — locked depression, rigid trauma patterns, calcified self-narratives — moving toward criticality is exactly what's needed. The medicine softens the rigidity. The pattern that's been stuck for years can briefly be seen as a pattern. The system can reorganize.
This is why, for treatment-resistant depression and similar conditions, psychedelics can produce changes that other treatments haven't reached. The traditional treatments often work within the existing patterns. Psychedelics work by softening the patterns themselves.
But the same medicines can be unhelpful, or actively harmful, for someone whose system is already drifting toward chaos. Someone in acute psychosis, severe dissociation, or active overwhelm doesn't need more entropy. They need more coherence, more structure, more containment. Psychedelics, in their case, can push the system further in the wrong direction.
This is part of why careful screening matters in psychedelic therapy. The medicine isn't right for everyone. It works particularly well for people whose suffering involves stuck patterns that need loosening. It's risky for people whose systems are already struggling to hold coherence.
What Happens at the Edge
When the brain is functioning at criticality — at the edge between order and chaos — something specific becomes possible.
Insight happens here. The moment a new pattern emerges from a previously unsolvable problem; the flash of seeing something clearly that had been opaque; the sudden recognition of a connection that had been invisible — these are the experiential signatures of a brain at criticality. The system is structured enough to integrate, flexible enough to discover.
This is what makes psychotherapy at depth so often involve sudden moments of clarity rather than gradual accumulation. The work, in some sense, is bringing the system to a state where new pattern-recognition becomes possible. The insight emerges from the criticality, not from accumulated effort alone.
It's also why some forms of suffering can change quickly, when conditions are right. Years of stuck depression can shift dramatically in a few weeks of effective psychedelic-assisted therapy. Decades of trauma patterns can begin to soften after a single experience that brings the system to criticality.
The change happens not because new information has arrived, but because the system's capacity to reorganize has been temporarily restored.
Why the Work Is About Balance, Not Fixing
This framework has changed how I think about clinical work, and I want to share that shift.
The traditional medical model approaches mental health by identifying a disorder and applying a treatment to fix it. Find the symptom. Match it to an intervention. Reduce the symptom. Move on.
The criticality framework suggests something different. The goal isn't to fix a broken system. It's to help a system that has drifted away from its natural balance find its way back.
Depression isn't a deficit. It's a state of excessive order.
Anxiety isn't a flaw. It's a state of excessive disorder, often produced by an over-active threat system.
Trauma isn't damage. It's a system that locked into protective patterns and lost some of its capacity for flexibility.
The work, in each case, is to help the system move back toward criticality — toward the balance of stability and flexibility that allows it to function well.
Different tools serve different drifts. Someone whose system has drifted toward too much order may benefit from interventions that introduce some healthy disorder — psychedelic therapy, new experiences, deeper emotional work, movement, expanded perspective. Someone whose system has drifted toward too much chaos may benefit from interventions that restore structure — grounding, routine, body-based regulation, nervous system stabilization, the careful containment of a steady therapeutic relationship.
Most people, in practice, need both. The work of therapy at depth often involves alternating between softening rigid patterns and stabilizing chaotic ones, with the goal of restoring the system's natural capacity to live at the edge.
What This Means for the People I Work With
If this framework lands for you, a few implications worth holding:
Your suffering is not a defect. It's a system that's drifted. What that means clinically is hopeful — drifts can be corrected. The same system that learned to over-order can re-learn flexibility. The same system that fragments under stress can re-learn coherence.
Healing is often about restoring balance, not removing something. This is a more generous and accurate framing than the medical model of disorder and treatment. You're not broken. You're temporarily off-center.
Different interventions serve different drifts. Knowing whether your particular pattern is more on the order side or the chaos side helps clarify what kind of work will actually help. Many people misdiagnose their own situation and try interventions that push them further in the wrong direction.
Psychedelics are a specific tool for a specific problem. They're remarkably useful for excessive order, and risky for excessive chaos. This is part of what careful psychedelic-assisted therapy is doing — assessing where someone is and whether a medicine that increases entropy is the right intervention right now.
Insight, breakthrough, and change live at the edge. This is where the work actually happens. Therapy at depth is often the slow work of bringing the system to a state where reorganization becomes possible — and then supporting whatever emerges.
A Closing Thought
The brain is the most complex object we know of in the universe. The fact that it manages, most of the time, to maintain itself in a state where consciousness can emerge — where flexible thought, emotional life, and the felt sense of being you all become possible — is itself remarkable.
When that balance is lost, suffering follows. The kinds of suffering that bring people to therapy are not random. They're the predictable patterns that emerge when a complex system has drifted from its natural equilibrium.
The work of healing, at its deepest, is the work of helping the system find its way back. Not back to some idealized state. Just back to the dynamic balance that allows life to feel like life again — coherent enough to make sense, flexible enough to surprise you, alive enough to matter.
This is what I think we're really doing in good therapeutic work. We're not fixing broken machines. We're helping living systems remember how to live at the edge of chaos — where everything important about being a conscious creature actually happens.
If you're sitting with patterns that have felt fixed for too long, or with chaos that's felt too overwhelming to organize, and you're curious about what integrative work could look like for you, you're welcome to book a consultation.
You Are a Controlled Hallucination: What This Means for Suffering and Healing
Neuroscientist Anil Seth argues that consciousness isn't passive reception of reality — it's an active, ongoing construction your brain produces moment by moment, including your sense of being a self. A therapist on what this framework reveals about trauma, depression, psychedelic therapy, and why understanding yourself as a process rather than a fixed thing opens up new possibilities for healing.
There's a quiet revolution happening in the science of consciousness, and most people haven't heard about it.
For centuries, we've assumed that perception works in a particular way. You open your eyes, light hits your retina, your brain receives that information, and you see the world. The brain is essentially a camera, recording what's out there.
This picture is wrong. Or at least, deeply incomplete.
What's emerging from cognitive neuroscience — and what the neuroscientist Anil Seth lays out in his book Being You: A New Science of Consciousness — is something stranger and more interesting. Your brain doesn't receive reality. It predicts reality, then uses your senses to correct its predictions. Most of what you experience as the world out there is actually a model your brain is generating, moment to moment, and adjusting based on sensory input.
Seth calls this controlled hallucination. The phrase sounds provocative, but it's surprisingly accurate. Hallucination, because the brain is generating the experience. Controlled, because the generation is constrained by what your senses are picking up from the world.
This idea matters far beyond consciousness research. It changes how we understand suffering, healing, trauma, and what psychedelic experiences are actually doing to the brain. I want to walk through why — because once you understand the framework, a lot of what happens in psychological work, and especially in psychedelic-assisted therapy, becomes clearer.
The Brain as Prediction Engine
The traditional model of perception was passive: information comes in, the brain processes it, you experience the result.
The newer model — sometimes called predictive processing — works the other way. Your brain is constantly generating predictions about what should be happening, then comparing those predictions to incoming sensory information. When the prediction matches reality, the experience feels seamless. When the prediction misses, your brain updates.
This sounds technical, but you can feel it in everyday life.
When you're walking down a familiar staircase and you miscount the steps, the brief lurching feeling — your foot going farther than expected, your balance unsettled for a moment — is your brain's prediction error becoming briefly visible. You expected solid ground. Sensation didn't deliver it. The mismatch produced that strange falling sensation.
When you read a sentence with a missing word, your brain often fills in the word automatically. The prediction is so confident that the absence doesn't even register at first. Magicians and optical illusions work by exploiting predictable predictions and producing experiences that contradict them.
Your everyday experience of the world — its colors, its solidity, its continuity — is largely your brain's confident model of what should be there, lightly corrected by what your senses actually report. Most of the time, the model is so accurate that you experience the world directly. But the experiencing is happening one layer in from reality.
What This Has to Do With You
Here's where Seth's framework gets personal.
If perception of the world is a controlled hallucination, so is your perception of yourself.
The felt sense of being you — your body, your thoughts, your sense of being a continuous person across time — isn't a thing your brain contains. It's something your brain constructs, continuously, from a combination of sensory signals from inside your body, memories, narratives about who you are, predictions about who you'll be, and the constant background processing of what it feels like to be alive.
This sounds destabilizing when stated bluntly. But it's actually how consciousness has always worked. You've never been a static entity inhabiting a body. You've been an ongoing process of self-construction the entire time. The continuity you feel is a kind of beautiful illusion, generated by your brain doing its job.
Seth's framing matters because it points at something useful: if the self is constructed, the construction can change.
The patterns you've been running for years — the harsh self-criticism, the chronic anxiety, the depressive self-narrative, the trauma responses — are not features of a fixed self. They're predictions your brain is making, repeatedly, about who you are and what's coming. They've become so confident, so automatic, that they feel like simply who you are.
But predictions can be updated.
Why Trauma Is So Hard to Reach With Words
This framework helps explain something many of my clients have struggled to understand about their own healing.
Trauma is, at its core, a prediction your brain made under conditions of overwhelming stress, that then got locked in. The world is dangerous. People are not safe. Closeness ends badly. My body is not okay. These predictions formed in the original moment, often when the system couldn't fully process what was happening. They became default models — the brain's confident assumptions about what to expect.
Years later, the world has changed. The original threat is gone. But the predictions are still running. Your brain is still generating experience based on a model that no longer matches reality, and the sensory information you're getting now isn't strong enough to update the model.
This is why insight alone often fails to change traumatic patterns. You can know, intellectually, that you're safe. The predictive model doesn't care. It was built to be robust against challenge, because at the time it formed, holding it tightly was a matter of survival.
What this framework suggests is that real healing requires not just new information, but new experiences strong enough to update the model. Experiences that the predictive system can actually feel, in the body, repeatedly, over time. The slow build of new predictions that compete with the old ones until eventually the old ones loosen their grip.
This is what trauma-informed therapy is actually doing, even when therapists don't describe it this way. Not just talking about what happened. Creating new experiences of safety in the body, in the relationship, in the room — experiences strong enough to begin to update the predictive scaffolding that trauma built.
Where Psychedelics Fit Into This Picture
Here's where Seth's framework connects to psychedelic therapy in a way that's both beautiful and clinically important.
The leading current model of how psychedelics work — developed by Robin Carhart-Harris and colleagues, and called REBUS, for Relaxed Beliefs Under Psychedelics — proposes that psilocybin, LSD, and similar compounds work by temporarily loosening the brain's predictive models.
In ordinary consciousness, the predictive system is strong, confident, and stable. The model of self and world it produces feels reliably real because it's been refined over years and is reinforced constantly. Even when the model is causing suffering, it's hard to shift because the brain trusts it so much.
Under psychedelics, this changes. The confidence of the predictions softens. The grip of the model loosens. Sensory information that would normally be ignored or absorbed into the existing model can suddenly be seen freshly. The structures that held the experience of self and world stable become temporarily fluid.
This is why people on psychedelics often describe seeing themselves and the world differently — sometimes radically so. Not because new information has appeared, but because the interpretive scaffolding through which everything was being filtered has temporarily loosened. The model of self can be glimpsed as a model. The story of who you are can be seen as a story.
And this is why psychedelic-assisted therapy may help with trauma, depression, and other patterns of suffering: not because the medicine fixes anything directly, but because it creates a window in which rigid predictive models can be updated by new experiences. The opening is temporary. What gets built during it — through preparation, support, and integration — is what can become lasting.
This connects directly to why so many practitioners now emphasize that the medicine alone isn't the treatment. The medicine softens the predictive scaffolding. The therapy and integration do the actual updating.
What This Framework Offers
A few implications worth holding:
Your suffering is real, but it's not a fixed feature of who you are. It's a pattern your brain is generating, with reasons. The pattern can change, though changing it usually requires more than insight alone.
The self isn't a thing to be fixed. It's an ongoing process. The work of healing isn't repairing a broken object; it's gradually shifting the patterns of construction. Different kinds of work — somatic, relational, contemplative, psychedelic-assisted — all participate in this shifting.
The body is central. Seth emphasizes that consciousness is deeply tied to interoception — the brain's perception of internal bodily signals. Your sense of being alive, of being you, is grounded in your body's ongoing regulation. This is why body-based work reaches places talk therapy can't. The predictive system that shapes your experience is built from bodily input as much as from anything else.
Psychedelics may have a specific role. Not as fixes, but as catalysts that temporarily loosen the predictive structures so that other work — therapy, integration, lived experience — can produce updates that wouldn't be possible otherwise. This is a more sophisticated and accurate picture than either "psychedelics are magic" or "psychedelics are dangerous." They are tools with a specific mechanism.
Healing is possible at a deeper level than symptom management. If suffering lives in predictive models, the deepest healing is at the level of those models themselves. Not just feeling better, but actually relating to yourself and the world from a different scaffolding. This is what people sometimes mean when they describe profound therapeutic experiences as feeling like they became a different person. The construction shifted.
A Different Way to Understand Yourself
The implication of Seth's work that I find most useful — both clinically and personally — is that you have never been the fixed thing you assumed you were.
The self you experience is a continuous act of creation. Your brain, in its remarkable way, is generating you, moment to moment, based on bodily signals and predictions and memories. The version of you that exists now is the latest iteration of a self that has been changing all along, even when it felt static.
This isn't nihilism. It doesn't mean you're not real. It means you're more alive than the old metaphor of a fixed self suggested. You are something happening, not something being. And the something that's happening can move.
For people who have lived inside a particular version of themselves for decades — a depressed self, an anxious self, a self defined by trauma — this framework opens a door. The self that has been suffering is one of many possible selves your brain could be constructing. Different inputs, different practices, different experiences can begin to construct a different one.
This is what the work of healing is, at the deepest level. Not removing something. Building something new — slowly, through repetition, through the body, through relationship, through whatever interventions help your predictive system update.
A Closing Thought
Anil Seth's framework doesn't solve the deepest mystery of consciousness. He's clear about that. We still don't know, at a fundamental level, why brain activity produces experience at all.
But the framework does something more useful for the question of how to live. It locates suffering and healing in a more accurate place — not in a fixed self that needs fixing, but in patterns of construction that can change. It connects the work of therapy, somatic practice, psychedelic-assisted experience, and integration into a coherent picture. It suggests that the strangeness of altered states is not strange at all — it's just the ordinary process of self-construction becoming briefly visible.
You are a controlled hallucination. That doesn't make your life less real. It makes it more available than the old picture allowed.
If you're sitting with patterns of suffering that have felt fixed for too long, and you're curious about the kinds of work — therapeutic, somatic, contemplative, psychedelic-assisted — that can actually shift those patterns at a deeper level, you're welcome to book a consultation.